![]()
Part I
BACKGROUND
![]()
1
INCIDENCE AND PREVALENCE OF DEMENTIA IN U.S. RACE AND ETHNIC POPULATIONS
Kala M. Mehta and Gwen Yeo
This edited volume covers the topic of dementia among different race and ethnic populations residing in the United States (US). As evidenced by the almost daily stories in the popular press, dementia is a tremendously important topic as one third of older adults in the US can expect to have the condition by the time they are 85 (Herbert, Weuve, Scherr, & Evans, 2013). There are many audiences who may be interested in learning about dementia in different race and ethnic groups. Understanding the scope may be important for clinicians in providing care, researchers in developing good research questions, policy makers in allocating resources, social workers and others working with caregivers, and older individuals and families from diverse populations trying to understand the cognitive decline with which they are struggling.
There is increasing recognition that dementia includes a range of neurocognitive disorders. In fact, dementia is not a single entity, but an overall term for conditions characterized by a decline in memory or other thinking skills that affect a person’s ability to perform everyday activities (Alzheimer’s Association, 2014). It includes a set of related clinical syndromes that may have different characteristics depending on type of neurological dysfunction or damage, risk factor profile, biomarkers, and stage of progression. Dementia carries substantial morbidity and mortality, as now one in three older adults in the US who die in a given year have been diagnosed with some form of dementia (Alzheimer’s Association, 2014).
It is not always clear which terms to use when describing dementia. The scientific terminology has changed since the first edition of this volume in 1996, most recently by the changes specified in the fifth edition of the Diagnostic and Statistical Manual of Psychiatric Disorders (DSM-5) published by the American Psychiatric Association in 2013. While the term ‘dementia’ is still commonly used in both scientific and lay publications, the more specific terms outlined by DSM-5 are sometimes preferred when precise diagnoses are needed. In contrast to the primary impairment category listed as “dementia” in DSM-IV, in DSM-5 it is “neurocognitive disorder” (NCD), which can be either major or minor and classified as either possible or probable. Subtypes were listed as Alzheimer’s disease, HIV infection, Parkinson’s disease, Huntington’s disease, prion disease, Lewy body disease, frontotemporal lobar degeneration, traumatic brain injury, vascular NCD, substance/medication-use NCD, or it can be unspecified (Foley & Heck, 2014). In clinical care, diagnosing the specific subtypes using DSM-5 criteria frequently involves neuroimaging, medical history, and neuropsychological testing (see Chapters 3–7 for more information on assessment). Often, however, in community-based settings with fewer resources and fewer highly specialized medical personnel, there is less opportunity to use neuroimaging and detailed diagnoses. Because the articles used as sources for prevalence and incidence data and related topics primarily use the terms “dementia,” “Alzheimer’s disease,” and “vascular dementia,” in contrast to specific neurocognitive disorders, those are the terms that will be used in this chapter and most of the volume.
Race and ethnicity are important social constructs. The terms are commonly used but lack scientific bases, and they are frequently used interchangeably. The categories used in this chapter and most of the scientific literature are based on the minority designations from the U.S. Census, which specify five populations as races: African American or Black, American Indian, Asian, Pacific Islander, and White. Although the term ‘ethnic group’ generally refers to a population with a common cultural background, as used in the U.S. Census, the term ‘ethnicity’ is applied to populations only with Hispanic/Latino ancestry; this category is also classified as minority along with the racial designations. Individual census respondents are asked to identify their race and also their ethnic background, i.e., whether or not they are Hispanic/Latino.1
Our goal in this volume is to describe the current state of knowledge on the impact of dementia among minority populations, to inform the scientific community of relevant gaps in the literature for specific groups, and to make information available to a wide audience of clinicians, educators, and policy makers so they can make evidence-based decisions about care for diverse patients. The populations included in this volume are those for whom there is information available, all of whom are ethnic minorities except for Chapter 9, on working with lesbian, gay, bisexual, and transgender individuals and families. Unfortunately, there are many other immigrant groups in the US that are not represented due to lack of published information.
Incidence and Prevalence
The question is frequently asked of the authors, “Is there a difference between minority populations in how often they get dementia?” The relative prevalence of dementia is important background information for the chapters on specific populations that follow, so its relative impact can be evaluated. To set the stage, the authors of this introductory chapter developed a systematic review examining dementia prevalence and incidence in English language literature among populations considered minority residing in the US. Those categories include Latino/Hispanic, African American, Asian, American Indian, and Pacific Islander (Mehta & Yeo, 2017). These minority categories can include many diverse populations, so in this chapter we disaggregate as much as the data allows. So, for example, in our review of Hispanic/Latino groups, we break down the information into Mexican Americans, Puerto Rican, Cuban, Caribbean Hispanic, and other Latino Americans. We disaggregate Asian categories as well, where data are available. The systematic review covered 114 studies from the 1980s to the present. As an update to that review, in this chapter we added data for four later studies with incidence information.
The amount of data on rates of dementia in different race/ethnic groups has grown dramatically since the first edition of this volume was published in 1996, and even since the second edition in 2006. Interpretation of this literature is difficult for many reasons – the most obvious is the lack of comparability between studies because they use different eligibility criteria such as age, and a variety of measures of dementia. Various screening instruments and various test batteries are used, some validated within the specific race/ethnic populations and some not.
Because there are no national datasets on the prevalence or incidence of dementia in the United States, available information for this chapter comes from regional studies, in some instances only on one race/ethnic group.
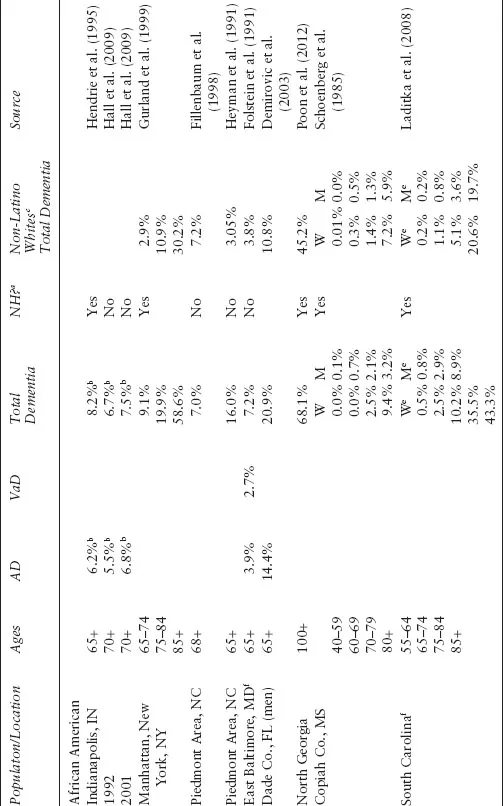
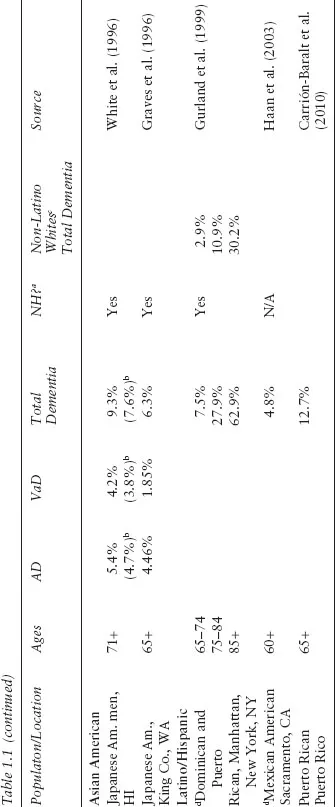
Figure 1.1 charts incidence studies, and Table 1.1 summarizes prevalence studies. In each instance, rates for non-Latino Whites are also shown from those studies which included them. We thought it important to include this group as a referent. Some may wish to refer to this group as Caucasian. For each population, we list incidence first, as it is a measure of the number of new cases of illness in a given population in a specific time period and is a better measure to compare across populations. We list prevalence next, as it refers to the total number of cases for a given population, and as such it is a better estimate for the purposes of health planning and provides a picture of the burden of disease in the population. It is used less often to compare across populations, as it is influenced heavily by disease duration, which varies between populations. To make incidence rates comparable across different racial/ethnic populations, the annual incidence was calculated from data in the respective studies; average annual incidence for populations was calculated for those in which there was more than one study.
Specific Populations
African American
Most of the literature on the rates of dementia among minority populations focuses on African Americans; articles reporting the prevalence or incidence of dementia among African Americans outnumber those for all the other populations combined.
Incidence
Annual incidence of dementia for African Americans ranged from 1.4% to 5.5%, with an average of 2.6% (standard deviation [SD] =1%), representing 14 studies (Evans et al., 2003; Fillenbaum et al., 1998; Gao et al., 2011; Gurland et al., 1999; Hendrie et al., 2008; Louis, Tang, & Schupf, 2010; Luchsinger, Tang, Stern, Shea, & Mayeux, 2001; Mayeda, Glymour, Quesenberry, & Whitmer, 2016; Muller et al., 2007; Perkins et al., 1997; Sanders et al., 2010; Shadlen et al., 2006; Yaffe et al., 2013).
In comparative studies of African Americans and non-Latino Whites, the incidence of dementia in African Americans ranged from 1.4 to 2.6 times that of non-Latino Whites (Gurland et al., 1999; Yaffe et al., 2013).
Prevalence
The studies reviewed that reported prevalence among African Americans vary according to dates of the studies (1985 to 2012), in age of the samples (≥40 to ≥100), methods of recruitment, whether nursing home residents were included, assessment instruments and procedures used, and how results were reported, as well as geographic areas where subjects were recruited. Prevalence ranges from <0.01% in 40- to 50-year-old women in Copiah County, Mississippi (Schoenberg, Anderson, & Haerer, 1985) to 68.1% in adults 100 years and older in Georgia (Poon et al., 2012). In the North Manhattan study, prevalence rates reported by age cohorts were much higher than in any of the other studies of African Americans. For example, 59% of those aged ≥85 were found to have dementia, compared to the four other reports of the same age, which ranged from 12% to 32% (Fillenbaum et al., 1998; Gurland et al., 1997; Hall et al., 2009; Hendrie et al., 1995; Laditka et al., 2008). Similar to the incidence studies, most comparisons of prevalence among African Americans and non-Latino Whites show higher rates of dementia among African Americans. Progression of Alzheimer’s disease (AD) was found to be slower among African Americans, and compared to Whites, African Americans with dementia are less often placed in a nursing home (Barnes et al., 2005; Schulz et al., 2010). Several reports now suggest that after a diagnosis of AD, African Americans live longer with the illness (Barnes et al., 2005; Fillenbaum, 2008; Helzner et al., 2008; Mehta et al., 2008).
Table 1.1 Prevalence of Dementia in Studies with Ethnic Minority Populations in the United States
Note
a Does the study include nursing home/institutionalized populations?
b Age standardized prevalence rate
c Prevalence in non-Hispanic white population if the study includes comparative data
d Ethnic background of majority of subjects
e Total of AD and VaD
f Population identified as “non-white” but generally interpreted to be African American
American Indians and Alaska Natives
Incidence
The only report of incidence among American Indians or Alaska Natives is from Mayeda and colleagues, who published data on the incidence of dementia in several populations in the Kaiser Northern California Healthcare System over 14 years of follow-up (Mayeda et al., 2016). Their findings suggest that the incidence of dementia in American Indians/Alaska Natives is high (2.8%), similar to African Americans, and nearly double the incidence in non-Latino Whites. It should be noted that this Northern California population of American Indians is probably highly urbanized and may not be representative of those in rural and tribal areas throughout the US.
Prevalence
No dementia pr...