![]()
CASE 1: ROBOTIC-ASSISTED RESECTION OF FIBROUS DYSPLASIA OF THE RIBS
Hiroko Nakahama and Wickii T. Vigneswaran
| Key Words |
• Robotic-assisted thoracoscopic surgery • Fibrous dysplasia • Chest wall tumor |
Introduction
Fibrous dysplasia is a skeletal disorder that replaces medullary bone with benign fibrous connective tissue. These tumors are typically asymptomatic but can present as a painful mass or with pathologic fractures. Radiographically, they appear as a fibrous bone deformity with fusiform expansion and cortical thinning [1,2]. Surgical resection is indicated for symptomatic lesions or lesions suspicious for malignant disease.
Traditionally, chest wall tumors are resected with a large thoracotomy, often necessitating reconstruction for large defects. Video-assisted resection has also been described in case reports; however, their use is limited by the bony chest wall anatomy [3,4,5,6]. The robotic system has the advantage of high-definition three-dimensional reconstruction of the dissection plane with fine motor maneuverability through small port sites. Here, we report successful robotic-assisted thoracoscopic resection of fibrous dysplasia of the ribs.
Case Report
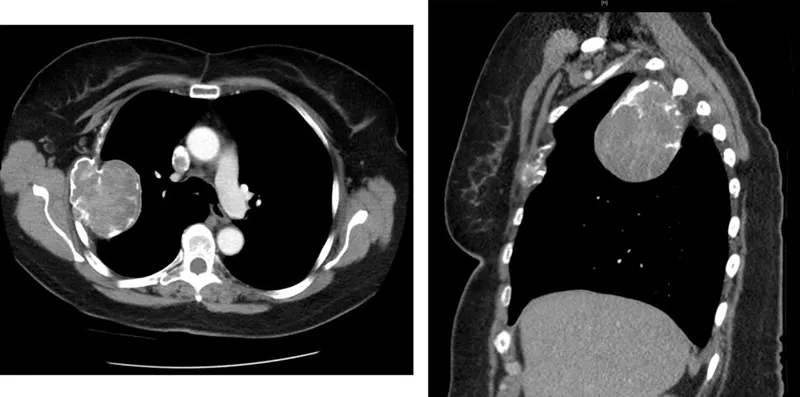
A 68-year-old female with fibrous dysplasia of the ribs presented with right-sided chest pain and difficulty breathing. She was diagnosed with fibrous dysplasia over 30 years ago and was clinically followed for the progression of the disease. With a serial computed tomography (CT) scan, she was found to have an interval increase in size of her tumors; the lateral third rib tumor measured 7 cm by 6 cm, and the 10th rib tumor measured 4 cm by 2.6 cm compared to 6 cm by 4.5 cm and 3.1 cm by 1.1 cm, respectively, 8 years prior (Figure 1.1). On physical exam, she did not have any palpable masses in her chest wall. Due to the expansile nature of the enlarging tumors, surgical intervention to exclude malignant degeneration was recommended to her.
The patient was given anesthesia and a double-lumen endotracheal tube was inserted for lung isolation. She was placed in a left-lateral decubitus position. A camera port incision was made in the subscapular area, and the second and third thoracoports were placed under direct visualization in the sub-mammary area and paravertebral area and the utility port in the ninth intercostal space at the anterior area of the second tumor. The robotic da Vinci Si surgical system was docked in the appropriate position.
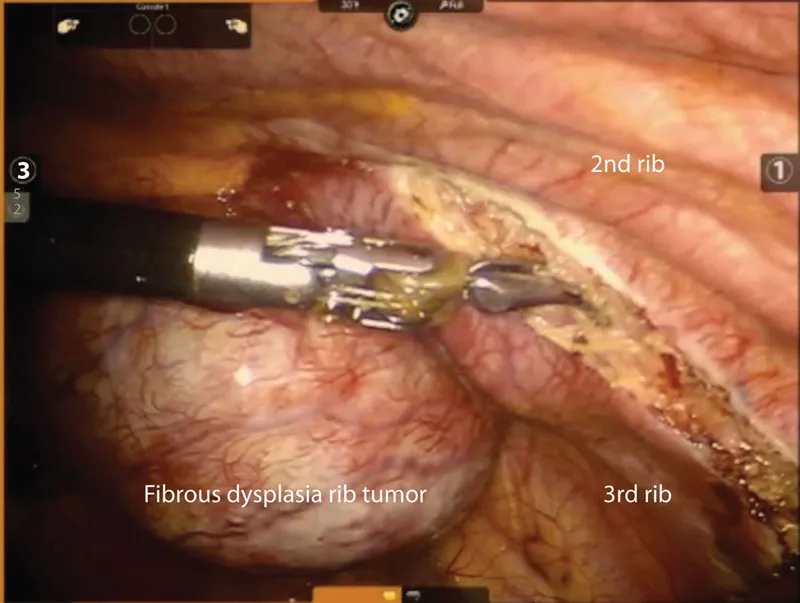
First, the resection of the large tumor on the third rib was performed (Figure 1.2). The intercostal resection was performed using bipolar and unipolar electrocautery. The ribs were divided on both ends using Dennis rib shears for an en-bloc resection of the tumors, preserving the chest wall muscles while removing adequate margin and mobilization of the tumor. The large mass on the third rib was then placed in an Endo-bag.
Next, the tenth rib intercostal space and neurovascular bundle was dissected with a similar technique using electrocautery. After the tenth rib was sheared, video-assisted thoracoscopic technique was utilized for resection of the remaining tumor on the tenth rib. Through a 3 cm skin incision over the tenth rib, the second tumor was removed and extracted through the incision site. The third rib tumor contained within the Endo-bag was then extracted through the same incision that was made to remove the tumor on the tenth rib.
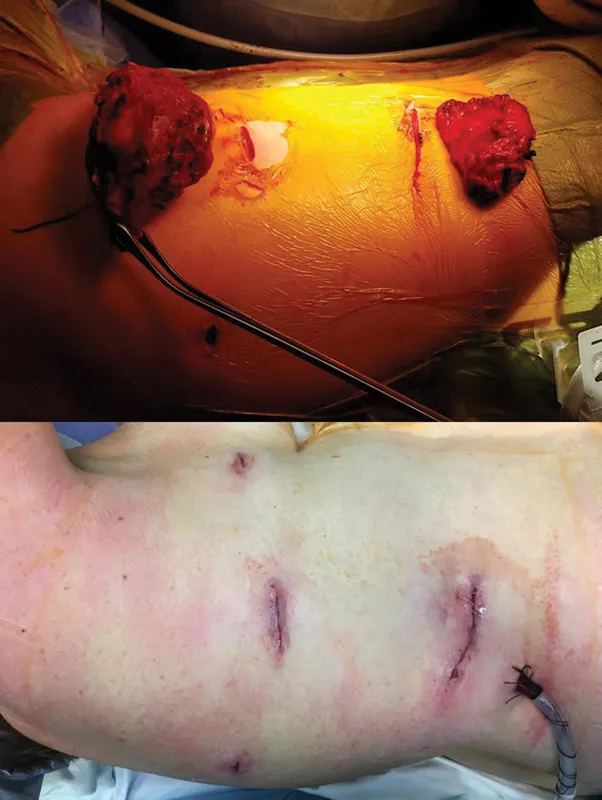
The patient recovered well from surgery and was discharged home on the following day. The large tumor on the third rib and the tumor on the tenth rib measured 9 cm and 5 cm, respectively, at their greatest dimension. The pathology report confirmed fibrous dysplasia for both tumors, and the edges showed increased cellularity resembling giant-cell reparative granuloma. There was no atypia or increased mitotic figures identified. At the one-week and two-month follow-ups, the patient remained without pain or signs of recurrent disease (Figure 1.3).
Comments
Fibrous dysplasia comprises approximately 30%–50% of benign bone tumors [1]. Fibrous dysplasia can be divided into two types: monostotic with one bone involvement and polyostotic with multiple bone involvement. Monostotic fibrous dysplasia occurs in approximately 70%–80% of cases and arises most commonly in the ribs, proximal femur, tibia, and skull [1,7]. Polyostotic fibrous dysplasia involves more than one bone and is closely associated with McCune-Albright syndrome [1]. Fibrous dysplasia arises sporadically and affects the ribs in approximately 6%–20% of cases [8]. Surgical resection is indicated when lesions become symptomatic and cause significant deformation, or when malignant disease is in question. Malignant degeneration occurs in approximately 0.5%–4% of cases [8,9,10].
Surgical management of chest wall tumors has traditionally been performed with a thoracotomy with wide local excision and chest wall reconstruction for defects greater than 5 cm [2]. This approach is associated with high morbidity caused by altered respiratory mechanics due to deformed chest wall architecture and perioperative pain. More recently, video-assisted thoracoscopic rib resection has been reported for various chest wall tumors [3,4,5,6]. Although this approach decreases the pain associated with a large thoracotomy and can preserve chest wall structure, the instrumentation is largely limited by chest wall anatomy and dependent on the location of the tumors.
Robotic-assisted thoracoscopic surgery for use in chest wall tumor resection has not been well described in literature. Robotic-assisted resection of the first rib for Paget-Schroetter syndrome has been reported [11,12]. A series of cases have demonstrated low rates of neurovascular complications in the setting of superior visualization of the operative field, minimized pain, and long-term patency of the subclavian vein [11,12].
Robotic-assisted thoracoscopic resection of chest wall tumors is a good alternative to thoracotomy or video-assisted thoracoscopic resection. This approach has the advantage of high-definition three-dimensional reconstruction with fine motor maneuverability for dissection through confined spaces. This method preserves the underlying muscular architecture of the chest wall, limiting the need for subsequent reconstructive procedures. The small incision and limited rib retraction significantly reduces perioperative pain and shortens the length of the hospital stay. The disadvantage of this approach is the cost of the robotic system, which is shared amongst multiple disciplines at our institution, and may also be offset by the decreased hospital stay and reduced use of analgesic medications. Although this case took 499 minutes to complete, as this was the first robotic chest resection case done at our institution, we anticipate the operative time can be significantly reduced with subsequent cases and training of ancillary staff.
Here, we describe the first robotic-assisted resection of fibrous dysplasia tumors of the rib with excellent results (Figure 1.4). This method can be applied for any benign lesion of the ribs and should be considered to reduce perioperative pain and morbidity associated with the traditional methods.
...