eBook - ePub
Advanced Consulting in Family Medicine
The Consultation Expertise Model
- 236 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Advanced Consulting in Family Medicine
The Consultation Expertise Model
About this book
What distinguishes the consulting of experienced family doctors from their newly qualified colleagues? The question is often frustratingly hard answer clearly or objectively: unlike many professions, family doctors face a dearth of clear expectations of what constitutes advanced practice, a lack of defined standards against which to evaluate it, and an absence of expertise-related professional training in which to develop it post-certification. The model of consultation excellence outlined in this book illustrates in practical terms how advanced consulting can be nurtured. It avoids tantalising value judgement such as 'excellence'. Instead, it describes behaviours in terms that can be observed day to day, providing a detailed picture of what constitutes advanced consulting behaviour, how family doctors can be helped to acquire these higher levels of expertise, and how changes in behaviour can be identified and evaluated. "Advanced Consulting in Family Medicine" is written in handbook form for easy access and use, and provides a vital vision of higher order family doctor consulting.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1 Introduction To The Consultation Expertise Model
What Is Advanced Consulting About?
‘Fulfilment and excellence should be the goals, and deserve to be the destiny, of anyone embarking on a Vocational Training Apprenticeship . . . The trouble is, “fulfilment” appears to be a will-o’-the-wisp; and despite our chasing it with a net made of objectives and checklists, “excellence” tantalisingly evades capture, no matter how fine the mesh.’1
Consulting: it’s what family doctors do every day, week in week out until it’s taken for granted. By some that is. For experienced doctors it appears easy: sit down, glance at the screen and, ‘Hello, how are you?’ Just as the skilled musician takes up an instrument, looks at the score and plays a perfect series of notes to make music that is personally idiosyncratic and yet moves others. Ask these experts to describe what they are doing and the answer may be something akin to, ‘I don’t know. I just do it’ – what Daniel Barenboim in the 2006 BBC Reith Lectures called ‘conscious naivety’. This is fine for reassured patients or music lovers but it is very frustrating for teachers. They like to know what’s going on and want answers to questions such as:
- What exactly do experienced family doctors do?
- What distinguishes expert family doctors from their colleagues?
It shouldn’t be such a mystery!
‘A diverse group of case studies illustrates the grounding of skill in physical practice – the hand habits of striking a piano key or using a knife; the written recipes used to guide the neophyte cook; the use of imperfect scientific instruments like the first telescopes or puzzling instruments like the anatomist’s scalpel; . . . Developing skill in all these domains is arduous, but it is not mysterious.’2
It’s about the way experienced doctors consult
We were prompted to explore these questions by people working as simulated patients in specialist training for family medicine. They studied, in great detail, recordings of patients made in daily surgeries in order to develop simulations. The simulation is subsequently used with doctors in training as well as by experienced practitioners.3 As the simulator recreates the same patient to each of these doctors, perhaps inevitably they make comparisons. They tell of being aware of the cogs going round in the heads of family doctor trainees, with cog rotation punctuated by pauses that resonate with messages such as, ‘What do I ask next?’ By contrast they describe consultations with more experienced doctors as seamless, easy, relaxed or sometimes even puzzlingly unpredictable. Hence the question: ‘What distinguishes the consulting of experienced family doctors from their newly qualified colleagues?’ At the time there appeared to be no easily available answer that could be used by medical educators. This book provides an answer.
Advanced Consulting presents a schematic representation of what expert family doctors actually do. It avoids tantalising value judgement such as ‘excellence’, but describes expert behaviours in terms that can be observed day to day. The Consultation Expertise Model, hereafter referred to as the Model, illustrates in practical terms how the quality of consulting performance may develop over the years, given time for reflection and a commitment to learn from experience.
It is not surprising that one question necessarily leads on to another. In most fields of professional endeavour there is a clear understanding of what constitutes best practice, together with appropriately staged training for those practitioners who aspire to reach higher levels of practice. This is exemplified in many secondary care specialisms. However, while family doctors may extend their expertise into areas of special interest or needs – minor surgery, sexual health or asylum seekers, for example – there is no universal expertise-related training available post certification or accreditation. Given the above, the Model seeks to provide a detailed picture of what constitutes advanced consulting behaviour, i.e. best practice. Furthermore, it seeks to establish how changes in behaviour can be identified and evaluated and how family doctors can be helped to acquire these higher levels of expertise.
As the ideas embedded in the Model came together it became possible to express them graphically in a circular format as can be seen in Figure 1.2. This allows the Model to be used as a tool to ‘map’ consultations. Consultation mapping is a familiar technique introduced by Pendleton et al.4 and elaborated by Tate.5 The circular ‘map’ generated using the Model is called a fingerprint.
It’s about capturing excellence in the consultation through ‘fingerprinting’
A fingerprint is a form of consultation capture directly related to the Model that diagrammatises behaviour observed at different performance levels – always case-specific. Fingerprints made according to the criteria of the Model provide evidence on which to base discussion of what happened, what might have happened and, had behaviour been different, prompt thinking about future intentions that can be included in a learning plan.
Please note – a consultation map plots how events during the consultation pass through predetermined domains (e.g. establishing reasons for attendance) over a period of time whereas a fingerprint presents a holistic record of skills demonstrated in the consultation as a whole.
Using paperwork in the Fingerprint Pack provided in Appendix 4, post-fingerprint discussions contribute to a continuing professional development (CPD) process that can be included in appraisal or revalidation folders. The facility to fingerprint consultations, as will be explained later, enables expertise development to be identified and evaluated. Fingerprints can be expressed in two different ways as shown in Figure 1.02.
It’s about how consulting expertise may be developed
Finding a way to identify what expert family doctors do turns out to be the easy part. Having obtained a picture of advanced consulting, the question of how to achieve the higher performance levels identified must inevitably follow. There is little point in dangling an enticing picture of what experts do in front of family doctors early in their careers when they are still consolidating and extending their range of experience. That would be frustrating and counterproductive for all concerned. Indeed the new doctor will have been in daily contact with expert behaviour by their trainer and mentor but will be unable to copy it because the gap between competent and expert behaviour is incomprehensible to them without an aid to analysis. Experts make it look easy. How can you copy a relaxed and knowing manner that has taken years of experience to achieve?
Ways to benefit from experience will be suggested later in the book. The Model itself incorporates detailed next-stage suggestions which, in conjunction with the fingerprinting process, can provide further direction and insight. In addition, three key approaches central to expert behaviour and usable for self-development or as taught workshops will be outlined as routes to an extended consultation expertise repertoire.
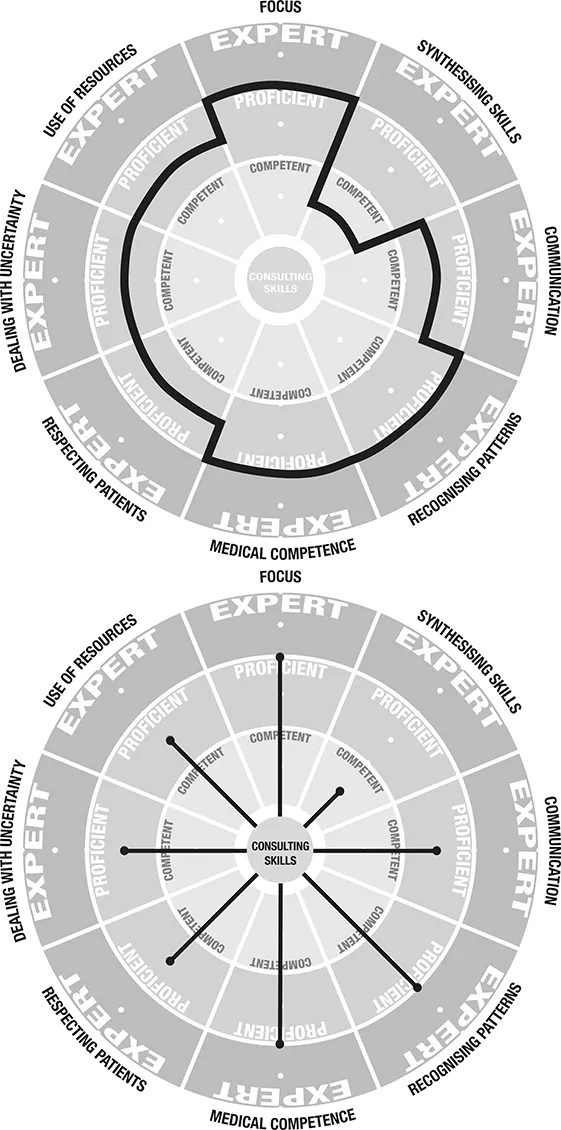
Figures 1.02a, 1.02b Case fingerprints: what they might look like
Advanced Consulting is about the development and growth of existing skills which have been learned by all family doctors by the time of certification.
At this point you may be thinking ‘Oh no, not something else to worry about’. However, the Model should be regarded not as another added pressure, but as a new way of looking at how existing skills are being used. Indeed, for many practitioners who have used it, it has evoked a revelation and provided the language for a reaction of, ‘Oh, that’s what I’ve been doing, is it?’
Advanced Consulting is written in handbook form for easy access and use. The Model and fingerprint process is explained stage by stage so that fingerprints can be made at home for personal reflection, for mutual exchange or within a practice organisation for dialogue between colleagues. Whichever approach is chosen, the resulting fingerprint can be used as evidence of professional development for the doctor who did the consultation.
In addition, the Model provides, maybe even provokes, a language and a vision of higher-order family doctor consulting for debate and celebration of professional skill. Another possible bonus is the prospect of acquiring internal staging posts to stimulate the intrinsic reward that can come from growth of expertise. In Roger Neighbour’s terms, as quoted at the beginning of this introduction, we have found this a fulfilling experience.
Finally, Advanced Consulting may be regarded as an exploration of expert doctoring for its own sake.
Consultation Expertise Model: Context
It is important to emphasise just how influential local factors have been in sustaining interest in this question of expertise. Three local context factors stand out. First, most of those involved have become familiar over the years with a nationally known consulting skill development framework devised and used locally for undergraduate training: the Leicester Assessment Package (LAP).6 LAP provides the basis for systematic training and assessment in the University of Leicester Medical School and is used by family doctor trainers with medical students. Patient simulators are also familiar with the methodology as they participate as patients in student action learning workshops.
Second, members of the group have been integrally involved in the development of patient simulations based on recordings of actual patients in real family doctor situations, not on written scenarios. As a consequence, the project group has had access to experienced simulators from the Leicester Simulated Patient Unit7 who are accustomed to looking at videotapes of experienced doctor consultations. Being able to compare different doctors consulting with the same simulated patient is a unique resource used frequently by the project group.
T...
Table of contents
- Cover
- Title Page
- Copyright Page
- Contents
- Foreword
- About the authors
- Acknowledgments
- List of Figures
- 1 Introduction to the Consultation Expertise Model
- 2 The Consultation Expertise Model
- 3 Fingerprinting
- 4 Uses of the Model
- 5 Advanced Consulting and the Model: Key Concepts
- 6 Practical Approaches to Developing Advanced Consulting Expertise
- Appendix 1: The Consultation Expertise Model: the developmental journey
- Appendix 2: The question of validity and reliability
- Appendix 3: The use of simulated patients
- Appendix 4: Fingerprint Pack
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Advanced Consulting in Family Medicine by Peter Worrall,Adrian French,Les Ashton in PDF and/or ePUB format, as well as other popular books in Medicine & Family Medicine & General Practice. We have over 1.5 million books available in our catalogue for you to explore.