eBook - ePub
Health Care Needs Assessment
The Epidemiologically Based Needs Assessment Review
- 172 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Health Care Needs Assessment
The Epidemiologically Based Needs Assessment Review
About this book
In the past 10 years spirituality and spiritual care have been much debated in professional healthcare literature, highlighting the need for a recognised definition of spiritual care to enable appropriate assessment of, and response to, spiritual issues. This accessible and highly relevant book surveys the numerous statements, guidelines and standards highlighted by these discussions, and equips healthcare professionals with the knowledge, skills and competence to provide the essence of spiritual care within their professional practice. Practical and evidence-based, this manual proves that delivery of good, professional spiritual care can build on intuitive human skills, and can be taught, learned, assessed and quantified. It gives readers the opportunity to move on from uncertainties about their role in the delivery of spiritual care by allowing them to asses and improve their understanding, skills and clinical practice in this area of care. Spiritual Care for Healthcare Professionals clearly grounds spiritual care in clinical practice. It is highly recommended for supporting academic study and encouraging healthcare practitioners to reflect on their practice and develop skills in spiritual assessment and care. Aimed at all healthcare professionals, it can be used by individual practitioners for continuing professional development as well as by academic staff developing educational programmes.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Health Care DeliveryAccident and Emergency Departments
B Williams, J Nicholl and J Brazier
1 Summary
Introduction
Hospital accident and emergency (A and E) departments manage major illness, minor illness, major trauma and minor trauma. Currently there is a move towards:
- having fewer commissioning agencies and major provider units
- treating minor conditions in less specialized facilities or in general practice
- role-sharing between doctors and nurses
- the establishment of regional centres to deal with major trauma.
This chapter reviews and forecasts the nature and volume of demand for A and E department services, assesses the costs and effectiveness of the component parts and presents three models of organization which may be appropriate for particular geographical circumstances.
Structures
There were 237 major hospital A and E departments in England in 1993 and 198 minor or peripheral units. A major unit served a 196 000 catchment population on average and some covered 600 000-900 000. 99% had a 24-hour radiology service, 98% a pathology service, 94% an intensive therapy unit (ITU) on site and half had associated short-stay facilities. Nearly half lacked computerized tomography (CT) scanning facilities. 15% were in hospitals having cardiovascular surgery and 12% in hospitals with neurosurgery. By 1994/95 there were 216 Type 1 A and E departments defined as having medical staff on site, each open 168 hours a week.
Minor and peripheral units are mainly in community hospitals and some are developing in closed or downsized general hospitals, or in extended primary care centres and polyclinics.
There are approximately 2500 doctors in A and E medicine. Around 265 are consultants. The number of consultants has increased considerably since 1990. The British Association for Emergency Medicine in 1993 estimated an average of 1:225 000 population, with the range among major provider units 1:60000-1: 500000. Designated nurse practitioners worked in 9% of major units and managed 3% of the new caseload.
Incidence of conditions giving rise to demand
With the introduction of more safety measures in the occupational environment and transportation, the incidence of serious injury from these sources is falling, but this is offset to some extent by the rise in criminal violence. The trend in incidence of minor conditions which make up the bulk of the work of an A and E department is unknown. The incidence of emergency medical and surgical conditions is increasing as the numbers and proportions of the middle-aged and elderly increase. This is demonstrable in respect of acute myocardial infarction and fracture of the neck of femur.
Activity
In 1994/95 there were nearly 12 million new attendances at A and E departments in England (246 per thousand population; regional range 188 to 295 per thousand). The numbers of new attendances are again increasing annually. Seven new attendances yield one reattendance on average. There were fewer than 35 000 first attendances annually in 54 Type 1 units, many serving scattered rural populations, but others were in the same or contiguous urban districts. Only 55 Type 1 units had 65 000 first attendances, or more.
The number and proportion of emergency admissions are increasing steadily. In some departments these patients are admitted through the A and E department, inflating new attendance numbers.
First attendance rates are highest among children, young adults and the elderly age groups, and among people in Social Class V. Inner-city A and E departments see proportionately more single people, commuters, migrants and the homeless.
A minimum data set is currently being adopted in A and E departments. No nationally representative information has hitherto been available on case-mix and case management. An overview of studies in individual units and areas suggests however that the new caseload of major A and E departments is mainly of low urgency. It includes:
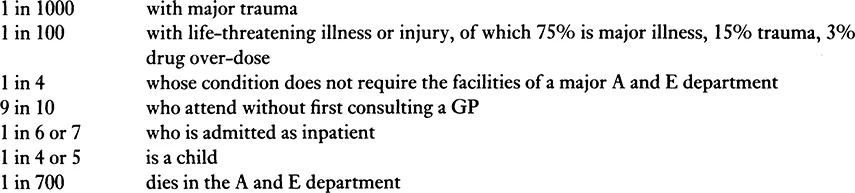
Demand is spread evenly over the days of the week and is higher during the summer. It is very low between midnight and 0800 (around 4%) but major trauma is more evenly spread, most cases presenting outside the well-staffed ‘office hours’.
Effectiveness
The effectiveness of A and E department services can be judged in terms of health gain or how patient demand is managed.
Structures
- Size Some studies show that major units in small hospitals are equally effective, clinically, as those in large hospitals for a range of conditions. US studies indicate better outcomes for major trauma in larger hospitals, with less frequent procedural mistakes and fewer avoidable deaths.
- Observation wards These are reported to be associated with improved processes of care in the elderly and patients with head injuries.
- Dedicated operating departments Delays in surgical intervention can lead to poorer outcomes in cases of major trauma.
- Triage In emergency conditions, pre-hospital triage to appropriate expertise and facilities improves outcomes. In hospital, triage into patient categories (hospital doctor, nurse practitioner, GP) improves the processes of care. Triage into degrees of urgency results in a tendency to ‘over-triage’ into more urgent categories, so that fewer admissions are actually seen urgently.
Clinical management
- Major trauma
- Regional trauma systems based on regional trauma centres have been shown to be effective in the US trauma setting. Such a system was shown not to be more effective nor cost-effective in the one situation in the UK where it has been evaluated.
- Specialists needed on site. Secondary transfer of cases, especially of head injuries, is associated with poorer clinical outcome. If neurosurgery is not available on site there should be locally agreed guidelines for the rapid transfer of cases to the appropriate facilities.
- Trauma teams. Early mobilization of senior medical (A and E, anaesthetist, surgical specialists) and nursing staff, with rapid assessment and resuscitation improves outcome.
- Advanced trauma life support (ATLS). The value of having a casualty team trained in ATLS is widely accepted.
- CT scanning. This is effective in improving the management and outcome for head injuries. The value for other injured parts is less clear cut.
- Radiographic service. A 24-hour radiographic service with senior radiological assessment improves outcome.
- Minor trauma
- Nurse practitioners (NPs). There is no evidence from prospective randomized, controlled trials that NPs manage minor conditions as, or more effectively than junior doctors.
- Minor injury units (MIUs). There is no evidence about the effectiveness of MIUs in managing minor trauma relative to major A and E departments or the general medical services.
- Major illness
- Disease management protocols. The value of following protocols for major medical conditions such as acute asthma and severe chest pain is established and they should be adopted.
- Basic life support. This improves survival chances in emergencies.
- Minor illness
- On-site GP services in major departments. Patients with minor conditions are managed comparatively more appropriately using on-site GP services rather than traditional junior casualty officers.
- Polyclinics and extended primary care centres. The effectiveness of these arrangements for managing minor illness and injury compared with other arrangements is unknown.
Costs
There are very few reports in the literature of relative costs of different methods of catering for accidents and emergencies, nor of the component parts of the service. In particular it is rare for the cost consequences of an A and E attendance to the health service or to the individual to be considered. Moreover there is currently no information system which provides the means of estimating the workload and hence the costs associated with each type of case.
Structures
- Size of department The average cost of a new attendance at an A and E department in England is about £45.00. The cost varies little and inconsistently among departments according to the annual number of new attendances.
- Amalgamation of units; full or partial closure of units No follow-up studies have been reported of the cost consequences to the health services. Whether or not hospital cost savings are achieved is not known. However when A and E department services are centralized additional costs fall on ambulance services and patients.
Clinical management
- Major trauma
- The additional cost of the first regionalized trauma system to be evaluated, including establishing and operating a regional trauma centre, was £0.5 million per annum. The cost consequences for contiguous A and E departments were small as the numbers of cases diverted were very small.
- Trauma teams, ATLS. Published data on the costs of these developments are not available.
- Major illness Data specific to the A and E department management of major illness are not available.
- Minor injury, minor illnesses The comparative costs of treating these conditions together with the other caseload in major A and E departments or of managing them in separate minor units are unknown. Where GPs are employed in major A and E departments to manage minor conditions there is a saving of more than one-third per case compared with management by doctors of senior house officer grade.
Cost-effectiveness
Estimates of the size of the health effects and the costs of different configurations of A and E services are generally either unreliable or non-existent.
Models of care
Three models are proposed which purchasers and providers will consider in relation to different geographical circumstances. There can be no gen...
Table of contents
- Cover
- Title Page
- Copyright Page
- Contents
- Foreword
- Preface
- Contributing Authors
- Introduction
- Accident and Emergency Departments
- Appendix I National Hospital Ambulatory Medical Care Survey Emergency Department Patient Record
- Appendix II Provider Minimum Data Set for A and E Departments with Computerized Systems
- References
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Health Care Needs Assessment by Andrew Stevens,James Raferty in PDF and/or ePUB format, as well as other popular books in Medicine & Health Care Delivery. We have over 1.5 million books available in our catalogue for you to explore.