1
Anatomy and differential diagnosis in head and neck surgery
Neeraj Sethi and Neil de Zoysa
Introduction
When assessing patients it is vital to formulate a differential diagnosis based on the initial history and examination. This guides decision-making in investigating patients swiftly and appropriately. Lack of investing thought into a differential diagnosis will lead to delays and unnecessary anxiety for the patient. Knowledge of the anatomy is essential to understanding what the pathology could possibly be. Whilst primary malignancy in neck lumps can occur (e.g. lymphoma, thyroid cancer or salivary gland cancer), the majority of malignant neck lumps are metastatic and immediate thought must be given to identifying the source of the primary tumour (which is likely to be in the upper aerodigestive tract).
Additionally, Occam’s razor suggests a unifying diagnosis to be the most likely correct diagnosis. This is often the case and makes sense in the setting of a patient with a sore throat, altered voice and a neck lump, where a differential diagnosis including hypopharyngeal carcinoma explains all symptoms. However, Hickam’s dictum must be remembered which states ‘a man can have as many diseases as he damn well pleases’, and there will always be patients with multiple pathologies.
Whilst the anatomy for each subsite of the upper aerodigestive tract is considered in more detail in each specific chapter, here an overview will be provided to ‘set the scene’ for a general assessment of the patient referred to a head and neck surgery clinic. As well as anatomy, the patient’s age, associated symptoms and risk factors for specific illnesses will guide differential formulation.
Anatomy
Triangles and levels
The neck is an anatomically complex but quite beautiful arrangement of vessels, cranial nerves, peripheral nerves, muscles and fascia.
For the purposes of clinical medicine and surgery, the neck can be broken down into triangles which are defined by palpable landmarks. This aids in both clinical examination and surgical planning.
From an operative point of view however it is equally important to understand the fascial planes of the neck. Generally speaking, these planes and their boundaries can be followed during surgery. By doing this, a clean operative field can be obtained ensuring complete and safe surgery via the relative ease at which important anatomy can be identified and preserved.
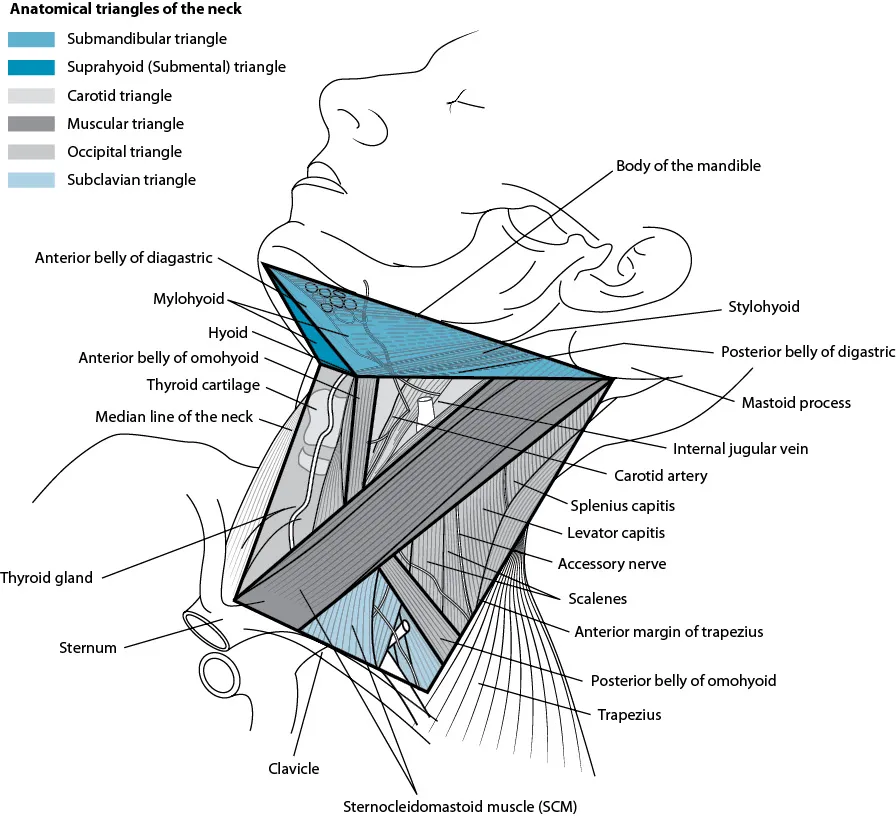
Important palpable bony landmarks are identified in Figure 1.1. These include the lower border of the mandible, the mastoid tip, the hyoid bone, the cricoid cartilage, the sternal notch, the clavicle and the anterior border of the trapezius muscle.
Figure 1.1 Triangles of the neck.
Using these landmarks, the neck can be divided into triangles as shown in Figure 1.1. The submandibular triangle has its superior border at the lower border of the mandible. It is then made up by the digastric muscle, which has two bellies running from the lesser cornu of the hyoid, one to the mastoid tip and one towards the digastric fossa of the mandible, just lateral to the symphysis (midpoint of the mandible).
Between the two anterior bellies of the digastric muscle and the body of the hyoid is the suprahyoid (submental) triangle.
The carotid triangle runs from the posterior belly of the digastric muscle to its insertion at the mastoid tip, then down the posterior border of the sternomastoid muscle, then up along the omohyoid muscle towards the lesser cornu of the hyoid. The omohyoid muscle is palpable in slim or muscular patients. As a surrogate, a line can be made from the lower two-thirds of the sternomastoid muscle to the lesser cornu of the hyoid.
The muscular triangle runs below this line (the omohyoid), the remaining sternomastoid muscle and the midline.
The occipital triangle is bordered by the posterior border of the sternomastoid muscle towards the mastoid tip, then along the anterior border of the trapezius, along the clavicle back to the sternomastoid. The subclavian (or supraclavicular triangle) is found within the posterior triangle, bounded by the inferior belly of omohyoid, the posterior border of sternocleidomastoid and the clavicle [1].
For the purposes of oncological description and axial imaging, the triangles are replaced by levels (see Figure 1.2 and Table 1.1). Levels are a more reproducible way of describing the location of pathology and should be used in preference to triangles in documentation, correspondence and discussion. In addition, the l...