eBook - ePub
Mental Health for Primary Care
A Practical Guide for Non-Specialists
- 220 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
'This book gives a 'bottom-up', practical overview of mental health. I have distilled psychological, biological and sociological background material and siphoned off anything that is not relevant to primary care. I aim to demystify the management of common problems and empower the reader to have a more rewarding and fun time at work and a better ability to cope with the ever-increasing demand and challenge of dealing with multiple physical and mental health issues often brought by a single individual to a time-limited consultation' - Mark Morris.This book provides an up-to-date guide to mental health for primary care workers who are not experts in the field. It is logically structured, providing a clear overview of causal factors before presenting individual conditions in a diagnostic hierarchy. Particular attention is given to areas where there has been a deficit in understanding or training, along with problems that are most frequently encountered and managed in primary care. Meanwhile, a Psychological Tools section introduces solid practical frameworks for managing mental health problems developed from cognitive behaviour therapy, solution-focused and motivational interviewing techniques. A selection of resources for patients is also included. It includes foreword by: Andrew Polmear MA MSc FRCP FRCGP; Former General Practitioner and Senior Research Fellow, Academic Unit of Primary Care, The Trafford Centre, University of Sussex, September 2008.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
PART ONE
Causation
CHAPTER 1
Vulnerability and resilience: personality
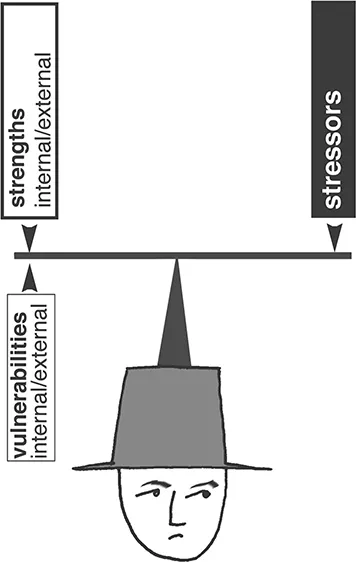
We all have vulnerabilities, strengths and resources. These can be external or internal. The fact that I have a relatively high genetic loading for the development of mental illness is an internal vulnerability. However, my training in mental health has made me very aware of this and I should be in a good position to spot the early signs of mental ill health. This is an internal strength. My openness with colleagues and family would help me to access support (external resources). Hopefully, in the face of a stressor the balance of vulnerabilities and strengths will be favourable. If not, neighbours may suffer the sight of me running down the street naked (something my relative did during a manic upswing). The more I think about it, the more important it is for me to bolster my resilience – the mental health of the whole neighbourhood is at stake!
In the field of medicine we often forget to consider the strengths of an individual. In the research, attention is given to weaknesses and vulnerabilities so that we can get a better understanding of the aetiology of mental illness. However, when it comes to moving out of illness or mental distress, strengths and resources are at least as important. Helping individuals to see that they are not the problem and that there is more to them than their difficulties can be very helpful in enabling them to make positive change. It can also be very refreshing for the practitioner.
Let’s take a journey from conception through to adulthood, looking at the factors which may have bearing on our mental health.
GENETICS
It would seem that there may be a genetic contribution to all mental illness. Bipolar affective disorder (manic depression) has the greatest heritability.* Family studies show that having a first degree relative with the condition makes you 8–18 times more likely to develop the condition yourself. Adoption studies confirm the genetic contribution by removing confounding environmental factors. To illustrate the point further, the lifetime risk of developing schizophrenia is 1% but having two first degree relatives with schizophrenia increases your risk to 46% (14% with one first degree relative). The genetics are complex and we cannot yet do anything about the loading once it is there. However, in primary care the family make-up is often known to us and we can be alert to genetic vulnerability in the hope of early identification of emerging mental health problems.
Genetics will also have influence over infant temperament as we will discover below.
BIRTH
Obstetric complications and perinatal hypoxia are associated with schizophrenia, particularly in males. Periventricular brain haemorrhages during labour and subsequently enlarged ventricles may be implicated.2,3
EARLY RELATIONSHIPS
Figure 1.1 serves as a useful summary – showing that healthy individuals have been provided with safety, security, lots of emotional warmth and a moderate amount of control.
Until the age of three: temperament and attachment
Temperament and ‘goodness of fit’
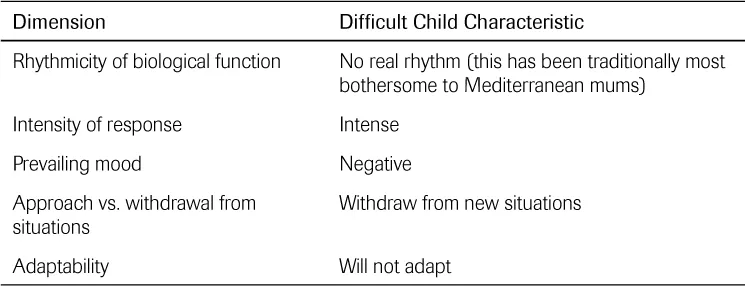
Many early characteristics are inborn. The infant’s behaviour can shape parental response, which will in turn influence the child’s emotional development. A child who likes cuddling and is easily soothed will promote feelings of competency in the carer and secure attachment will be promoted. The child who stiffens, wriggles and continues to cry when picked up for comfort will make the parent feel inadequate and rejected. There can be negative emotional and behavioural consequences when the child’s temperament and family characteristics do not fit nicely together. Thomas and Chess in the 1960s and 1970s found that particular characteristics were more likely to remain stable over time than individual characteristics. These clustered together to define the ‘difficult child’4 – outlined in Table 1.1.

FIGURE 1.1 Early relationships
TABLE 1.1 Difficult child
Attachment theory (Bolby,5 Ainsworth6)
Attachment theory states that the clinging behaviour which young children display towards their parents is normal and biologically determined, has particular characteristics, and is especially important in psychosocial development. Selective clinging to one person is understood as evidence of an individual’s first close personal relationship and it is held that the experience of that relationship will govern the quality of subsequent close relationships throughout life. The quality of attachment will influence future physical and psychological health with an effect on stress regulation mediated by the hypothalamo-pituitary-adrenal axis.7
At an average age of about six or seven months, children start to show attachment behaviours, which indicate that they are becoming psychologically attached to another person, usually their mother.
The attachment figure is usually someone who has had a lot to do with the baby in terms of play and comforting; feeding is not the crucial element and breast or bottle feeding is simply irrelevant. Even harsh physical treatment or battering is compatible with the development of an attachment to the abuser; it is the intensity of the interaction that matters. Nor is the amount of time spent with a person crucial; what matters is the intensity of social interactions. Working mothers are quite able to elicit attachments from their infants as long as they do things with them at some time during the average day. In practice the first attachment figure is nearly always the baby’s mother (or attachment is formed equally with mother and father). After the first attachment, a few other attachments are likely to be formed, particularly to the other parent, but do not have the intensity of the first one.
1 Normal attachment formation
The development of secure affectional bonds in early childhood makes it much more likely that an attitude of trust and optimism in personal relationships will persist in later life.
Normal attachment behaviours compatible with secure attachment formation are identifiable in routine consultations.
In the child normal attachment behaviours comprise:
➤ separation anxiety: crying when mother leaves the room; calling for her; crawling or toddling after her. Can interfere with settling at night. Some children find that they can deal with it by having a cuddly toy, known as a comfort object or transitional object such as a blanket or teddy bear. Their existence does not indicate insecurity
➤ clinging hard when anxious, fearful, tired or in pain, hugging, climbing onto her lap
➤ talking and playing more in her company
➤ using her as a secure base from which to explore
➤ stranger anxiety: wariness towards and shyness of strange people which promotes clinging to the attachment figure in their presence.
Attachment behaviours are intensified by:
➤ anxiety
➤ tiredness
➤ illness.
The mother or carer will be observed responding sensitively to the child’s needs, providing a sense of security. This promotes adequate resolution of separation anxiety.
Ordinarily speaking, a child gradually learns to tolerate separations so that separation anxiety wanes over the pre-school years, although it will still appear at times of distress and pain in young schoolchildren.
2 Abnormal attachment formation
A failure to develop affectional bonds may result in a lack of basic trust with resulting shallowness, suspicion and selfishness in future relationships (and remember this may include the individual’s relationship with you!).
It can sometimes be difficult to distinguish between unstable attachment formation and a self-sufficient child. The child may appear very friendly to the examining doctor but closer questioning or longer acquaintance reveals that he or she does not discriminate between familiar and unfamiliar adults in terms of seeking comfort and affection. Although appearing intimate (sitting on your lap, offering kisses), the relationship is superficial and easily broken by separation without any separation anxiety.
The best test is asking the mother if she feels emotionally close to her child
Parental and child factors can lead to abnormal attachment formation. Abnormal attachment patterns have been classified, but I can never remember them. Remembering the following influences may be more useful.
Parental factors
Harshness, coldness or rejection on the part of the parent can promote abnormal attachment behaviour and a poor prognosis for future antisocial behaviour. The situation can be improved if the parent can be persuaded to act in a more sensitive, affectionate and child-centred way, but this is not easy.
When attachment behaviours fail to develop adequately the long-term outcome is often poor with a general difficulty forming and sustaining close relationships, a difficulty learning social rules and a propensity in adult life to aggressive, promiscuous behaviour. These ‘immature’ adult personality traits fall into the diagnostic categories of psychopathic (antisocial); emotionally unstable (‘borderline’) personality disorders, and are discussed in Chapter 9.
Child factors
In some instances insecure attachment reflects elements in the child’s personality; wriggly children who do not want to hang around on the parental lap for cuddles even though the parents are loving and affectionate. Such a pattern has a good prognosis as long as the parents can accept their child’s individuality. There is no strong link with aggressive behaviour.
A bit of both
Children who are chronically clingy and obviously ambivalent to their mother, being actively cross with her following the briefest separations, can result from an unfortunate mix of the child’s temperament and mother’s state of mind or personality. A depressed and irritable mother, for instance, may be short-tempered with a child and her rejecting attitude promotes further clinging by the child. A mother with an immature personality may find herself unable to separate out her needs from the child’s and turn to the child f...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Contents
- Foreword
- Preface
- About the author
- Acknowledgments
- Background concepts
- Part One Causation
- Part Two Problems
- Part Three Psychological tools
- Part Four Patient resources
- Appendices
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Mental Health for Primary Care by Mark Morris,David Rogers in PDF and/or ePUB format, as well as other popular books in Medicine & Family Medicine & General Practice. We have over 1.5 million books available in our catalogue for you to explore.