What’s in It for the Patient?
Patients: The only reason that any healthcare system exists, yet so often considered merely as an afterthought. As healthcare providers, we sometimes get so caught up in our day-to-day activities that we completely forget that we are there to serve our patients. Those same patients that are the lifeblood of the healthcare system are beginning to act more like consumers. It’s partly being driven by the proliferation of high-deductible health plans that put more of the cost burden on the patient in exchange for lower monthly fees. We have also become a nation seeking instant gratification, information at our finger tips and options to do things where and when we want to do them. The millennial generation is known as “digital natives,” meaning they’ve never known a world without computers and the Internet. They are inherently tech-savvy, seeking services on their own terms and are quickly becoming a significant consumer of health services. It’s fair to say that millennials will demand the same types of services offered by other industries; healthcare systems that can provide that type of experience will thrive and those that can’t, well…they won’t.
Technology has been able to satisfy the needs of patients in just about every other industry. Remember paper airline tickets? How about calling to schedule a dinner reservation? Deposit a check into your bank account? Buying CDs in a music store? Heck, most people don’t even get a newspaper anymore. All of these activities can now be accomplished with the phone in your pocket. Why would our patients expect anything less of their local health system?
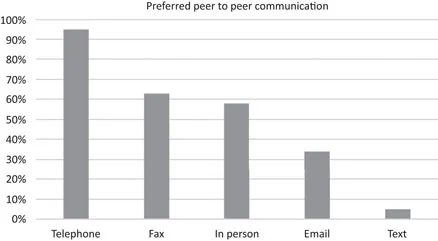
The current state of affairs within the healthcare system is far from the accessibility patients experience in other parts of their lives. While most health systems now have an Electronic Health Record (EHR) system, it was frequently implemented modeling an existing paper system. Oftentimes health systems implemented their EHR to take advantage of US government incentives for “meaningful use” of electronic health information. (We will explore the financial ramifications of this later in this book.) You would be hard-pressed to find many health systems today that allow you to schedule an appointment online, have access to your medical records, or get your test results electronically. And if you want to do some research to find out how much a test or procedure will cost you, you’d be out of luck as well. A physician’s survey conducted in 2012 concluded that 63% of physicians still preferred to communicate using a fax machine,1 as shown in Figure 1.1.
Figure 1.1Fax machines continue to live on in many healthcare settings.
The fact that we are still using a dinosaur (fax machine) to send mission critical documents like referrals and prescriptions (often printed off and scanned back into an EHR) should give anyone who interacts with the healthcare system pause. When patients realize how far behind the times their healthcare provider really is, they begin to question the competency of the system as a whole.
If you are still using technology from the 1980s, how can I trust you with my health?
How can we leverage an EHR system to create a better experience, with better outcomes? Let’s explore some of the ways that a modern EHR system can help bring the US healthcare system into the twenty-first century and bring value to the most important part of the healthcare system: patients.
A More Seamless and Safer Experience
Have you ever had an encounter with a healthcare provider and have been asked the same questions about your demographics and health that you just answered in another setting within the same health system? Has it ever happened in the same office? I think we have all had an experience like this! Sometimes these checks are performed as part of a protocol to ensure safety and accuracy (Are we working with the correct patient?), but a lot of times, they are done because there is not a common EHR, and the systems don’t “talk.” This reminds me of a story from a colleague who brought his son into a health system for treatment of a broken arm. He was admitted into the emergency room and asked the typical battery of questions upon check-in: What is your name? What is your birthdate? What brings you to the emergency room today?, etc. Enter the nurse: What is your name? What is your birthdate? What brings you to the emergency room today?, etc. Enter the physician: What is your name? What is your birthdate? What brings you to the emergency room today?, etc. Then on to radiology, and so it continues. After the fourth set of questions, his son looked at my colleague and said “They don’t have very good memories, do they dad?” This was a rather harmless example, and some of the questions are part of the safety protocol. Imagine, however, this was an 85-year-old man who was taking 24 different medications and he had to answer the question “What medications are you currently taking?” multiple times in multiple settings. This is where an EHR can really help.
Adverse drug events (ADEs) are usually caused by conflicting prescriptions or overdoses that lead to patient harm. It has been labeled a serious public health problem by the Centers for Disease Control (CDC),2 who list the following key facts:
82% of American adults take at least one medication and 29% take five or more.3
700,000 emergency department visits and 120,000 hospitalizations are due to ADEs annually.4
$3.5 billion is spent on extra medical costs of ADEs annually.5
At least 40% of costs of ambulatory (nonhospital settings) ADEs are estimated to be preventable.5
Studies have estimated that 2.4–3.6% of hospital admissions are caused by ADEs, of which up to 69% would have been preventable.6
A study at Boston Children’s Hospital found that by using EHR medication reconciliation tools, the providers were able to reduce medication errors by 58%.7 Since the EHR had a list of the patient’s preadmission medications already in the system, the providers could display the existing medications list on a split screen while generating a new list on the other screen so that they could see any conflicting prescriptions at a glance. Reducing or eliminating ADEs is a very complex and daunting task for the healthcare system.
Having an EHR in place is a step in the right direction, but there are also many process-related changes that need to be in place to completely error-proof the system for patients. The Agency for Healthcare Research and Quality (AHRQ), a division of the United States Department of Health and Human Services, has proposed the strategies shown in Table 1.18 to reduce ADEs.
Table 1.1Strategies to Prevent Adverse Drug Events Stage | Safety Strategy |
Prescribing | Avoid unnecessary medications by adhering to conservative prescribing principles Computerized provider order entry, especially when paired with clinical decision support systems Medication reconciliation at times of transitions in care |
Transcribing | |
Dispensing | Clinical pharmacists to oversee medication dispensing process Use of “tall man” lettering and other strategies to minimize confusion between look-alike, sound-alike medications |
Administration | Adherence to the “Five Rights” of medication safety (administering the Right Medication, in the Right Dose, at the Right Time, by the Right Route, to the Right Patient) Barcode medication administration to ensure medications are given to the correct patient... |