eBook - ePub
The Junior Doctor's Guide to Cardiology
- 184 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Junior Doctor's Guide to Cardiology
About this book
'The transition between medical student and junior doctor is both stressful and demanding. The learning curve is extremely steep, and even more so in the world of specialist medicine - Senior doctors expect a lot of their juniors and, as a result, people often feel out of their depth and may feel too embarrassed to tell their seniors when they don't understand something - ' - from the Preface Boost your confidence. This is a user-friendly manual for the junior doctor. Concise and easy to read, it is invaluable for day-to-day clinical cardiology while out on the wards. It provides a logical, stepwise guide through the more common problems encountered in cardiology and assists with clinical practice and decision making. Complications, prognoses and comprehensive explanations of investigations aid in understanding why certain tests are requested and how to interpret their results. The Junior Doctor's Guide to Cardiology helps you to make informed, confident decisions and gives you the assurance to optimise your time in cardiology. When I first entered medical school, a very wise senior tutor said to me, 'Collins, learn the basics and you won't go far wrong!' The problem is in defining the basics and how to identify them. I am sure this book will help you and hopefully entice you into the wonderful and expanding world of cardiology - good luck and don't forget 'learn the basics!' From the foreword by Peter Collins
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Medical Education1
Targeted cardiovascular examination
General appearance
The ‘end of the bed test’ is essential. Does the patient look well or unwell? If they look unwell, it is important to assess them according to the AB C format.
Follow the usual order of inspection, palpation, percussion and finally auscultation, but think logically about underlying diagnoses rather than just going through the routine.
Vital signs
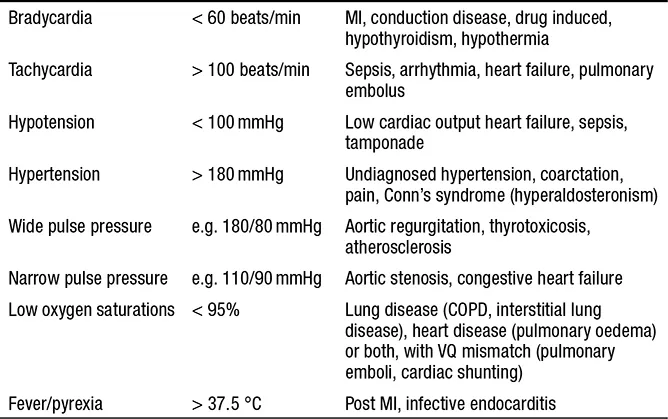
Pulse, blood pressure, temperature and oxygen saturations will often be available before you examine the patient. Observe for signs of haemodynamic compromise. Weight is an important factor for patients with heart failure, and should therefore be measured before breakfast every day to look for a trend.
Peripheral stigmata of cardiovascular disease
Is the patient comfortable? Consider their position. Are they breathless, in pain, coughing or cyanosed? Do they have a normal body habitus?
Hands
- Tar staining indicates that the patient smokes.
- Finger clubbing and central cyanosis are associated with congenital heart disease. Clubbing may also be seen in endocarditis.
- Looks for signs of hyperlipidaemia.
TABLE 1.1 Vital signs and their diagnostic considerations
- Signs of infective endocarditis are common if you look carefully. They include:
- — splinter haemorrhages (black streaks under the fingernails)
- — Janeway lesions (painless macular lesions on the palms or soles)
- — Osler’s nodes (painful red lesions, usually on the pulps of the fingers and toes).
Face
- Central cyanosis (pulmonary hypertension, intra-cardiac shunt).
- Signs of hyperlipidaemia – xanthelasma are soft yellow plaques around the eyelids, which are associated with lipid disorders.
- Poor dentition predisposes to endocarditis in patients at risk. It is also associated with ischaemic heart disease.
Scars
These often provide a clue to the type of previous surgery.
- Midline sternotomy – any cardiac or thoracic surgery. In the case of CABG, look for where the grafts have come from (saphenous veins, radial arteries).
- Subclavicular – devices (pacemaker, ICD).
- Neck – carotid endarterectomy, although increasingly this is an endovascular procedure (i.e. there is no scar).
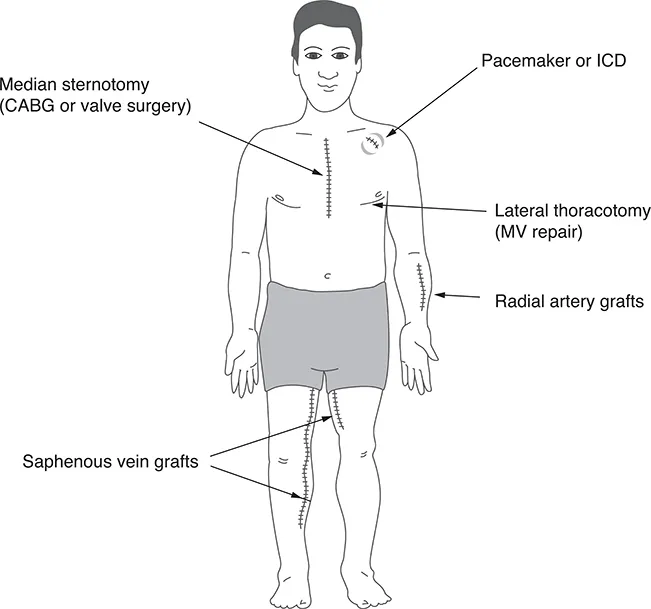
FIGURE 1.1 Schematic diagram of typical surgical scars in the cardiac patient.
Cardiovascular examination
Pulse
Note the rate, rhythm and character. Feel the foot pulses. Are they present and equal? If not, consider peripheral vascular disease, coarctation or aortic dissection.
Blood pressure
Record this from the left and right arm if you suspect dissection or coarctation.
Apex beat
LV enlargement pushes the apex down and out, making it harder to feel. RV enlargement brings the apex closer to the chest wall, creating a ‘heaving’ character.
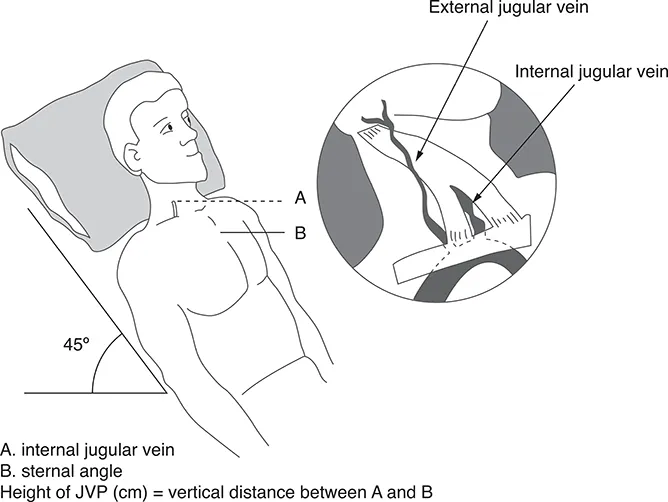
FIGURE 1.2 Assessing the jugular venous pressure.
Jugular venous pressure (JVP)
Look for obvious pulsations at the neck. Distinguish the JVP from the carotid pulse by its double waveform or by obliterating it with gentle compression. Conditions that can be diagnosed from the JVP include the following:
- heart failure
- tricuspid regurgitation (prominent ‘v’ wave)
- heart block (cannon waves – intermittent large ‘a’ waves)
- pulmonary hypertension (prominent ‘a’ wave)
- constrictive pericarditis (paradoxical fall in JVP on inspiration).
Heart sounds and murmurs
Listen for additional heart sounds as well as the loudness of each heart sound. It is important to detect severe valve lesions. In which position is it loudest? Is it systolic or diastolic? This will be covered in more detail later, but typical findings are as follows:
- Aortic stenosis: ejection systolic murmur radiating to the carotids. A quiet S2 and narrow pulse pressure indicates severe stenosis.
- Aortic regurgitation: early diastolic murmur at the ULSE. If severe, it can be heard at the upper right sternal edge as well.
- Mitral stenosis: diastolic murmur at the apex.
- Mitral regurgitation: pansystolic murmur audible into the axilla.
- Tricuspid regurgitation: pansystolic murmur at the ULSE, raised JVP, and pulsatile liver.
Lungs
Always listen to the lung fields for wheeze and crackles.
- Fine inspiratory and expiratory crackles – typical of pulmonary oedema.
- Fine end-inspiratory crackles – pulmonary fibrosis (check whether the patient is on amiodarone).
- Wheeze – asthma or heart failure.
Ensure that you percuss for pleural effusions, which may occur in the presence of heart failure.
Abdomen
Feel for an enlarged liver in right heart failure or tricuspid regurgitation (when it may be pulsatile). A splenic tip may be palpable in the context of endocarditis. Feel for an abdominal aortic aneurysm.
Peripheral oedema
Check the extent of oedema (e.g. ascertain whether there is sacral or perineal oedema). Consider other causes of lower limb swelling, including lymphatic or venous obstruction, low albumin levels or pelvic obstruction.
Vascular system
Ischaemic heart disease is closely linked to other atherosclerotic diseases, such as peripheral vascular disease, cerebrovascular disease and renovascular disease. Be aware that other systems may be affected when examining and taking a history. For example, if a patient presents with ‘new’ atrial fibrillation, consider peripheral embolisation, TIA or stroke, and bowel ischaemia.
Table of contents
- Cover Page
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Foreword
- Preface
- About the authors
- List of abbreviations
- 1 Targeted cardiovascular examination
- 2 Assessing the patient with chest pain, shortness of breath, syncope and palpitations
- 3 Successful ward rounds in cardiology
- 4 Safe prescribing in cardiology
- 5 Introduction to specialist investigations
- 6 Primary and secondary prevention of cardiovascular disease
- 7 Ischaemic heart disease
- 8 Heart failure
- 9 Atrial fibrillation and flutter
- 10 Tachyarrhythmias
- 11 Bradyarrhythmias
- 12 Valvular heart disease
- 13 Endocarditis
- 14 Hypertension
- 15 Aortic syndromes
- 16 Cardiogenic shock
- 17 Myocardial and pericardial disease
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Junior Doctor's Guide to Cardiology by Ian Mann,Christopher Critoph,Caroline Coats,Mann Ian,Critoph Christopher,Coats Caroline in PDF and/or ePUB format, as well as other popular books in Medicine & Medical Education. We have over 1.5 million books available in our catalogue for you to explore.