![]()
RESOURCES SECTION
Contents
1 Making connections -the synapse
By Dr Eric H. Chudler
This article apperas at: http://faculty.washington.edu/chudler/synapse.html
Reproduced with permission
2 Action potential
By Dr Eric H. Chudler
This article appears at: http://faculty.washington.edu/chudler/ap.html
Reproduced with permission
3 Pathophysiology of acute pain
By Sosnowski M, Pain Digest, (1994) 4(2): 100-105
This article appears at: http://www.pain.com
Reproduced with permission of the Dannemiller Memorial
Educational Foundation
4 Management of the individual with pain
Reprinted from Gersh R M and Echtemach J L, APT A Continuing Ed Series,
No.I ‘Management of the Individual With Pain, Part 1: Physiology and
Evaluation‘, PT-Magazine of Physical Therapy, December 1996.
This article also appears at: http:www.apta.org
Reproduced with permission of the American Physical Therapy Association.
5 Acupuncture, a brief introduction
This article appears at: http://www.acupuncture.com/Acup/Acupuncture.htm
6 Antidepressants and chronic pain
By McQuay HJ and Moore RA, (1997) British Medical Journal,
314:763 ( 15 March)
This article also appears at: http://www.bmj.com
Reproduced with permission
7 How to hit pain before it hurts you
By professor Clifford J. Woolf.
This article first appeared in MRC News, summer 1995, edition No.67.
Reproduced with permission
![]()
Resource 1
Making Connections — The Synapse
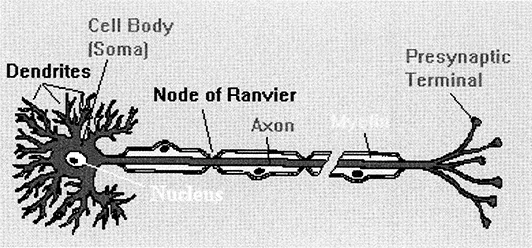
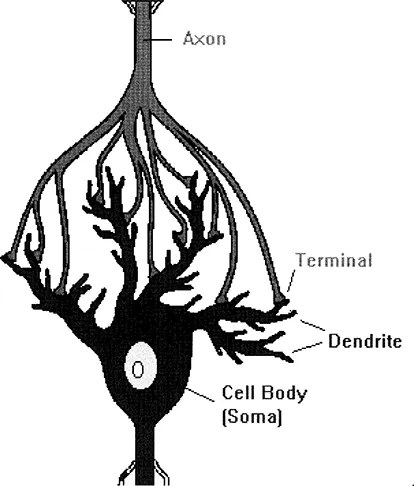
Neurons have specialized projections called dendrites and axons. Dendrites bring information to the cell body and axons take information away from the cell body.
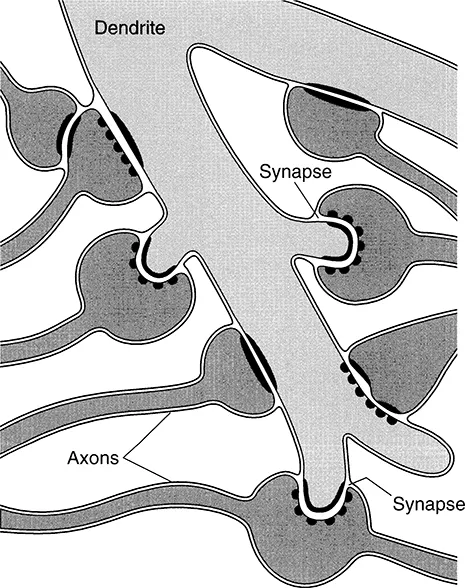
Information from one neuron flows to another neuron across a synapse. The synapse is a small gap separating 2 neurons. The synapse consists of:
a presynaptic ending that contains neurotransmitters, mitochondria and other cell organelles,
a postsynaptic ending that contains receptor sites for neurotransmitters and,
the synaptic cleft: a space between the presynaptic and postsynaptic endings.
Electrical Trigger for Neurotransmission
For communication between neurons to occur, an electrical impulse must first travel down an axon to the synaptic terminal.
Neurotransmitter Mobilization and Release
Here at the synaptic terminal (the presynaptic ending), the electrical impulse will trigger the migration of vesicles (the red dots in the figure to the left) containing neurotransmitters toward the presynaptic membrane. The vesicle membrane will fuse with the presynaptic membrane releasing the neurotransmitters into the synaptic cleft. Until recently, it was thought that a neuron produced and released only one type of neurotransmitter. This was called “Dale’s Law”. However, there is now evidence that neurons can contain and release more than one kind of neurotransmitter.
Diffusion of Neurotransmitters Across the Synaptic Cleft
The neurotransmitter molecules then diffuse across the synaptic cleft where they can bind with receptor sites on the postsynaptic ending to influence the electrical response in the postsynaptic neuron. In the figure on the right, the postsynaptic ending is a dendrite (axodendritic synapse), but synapses can occur on axons (axoaxonic synapse) and cell bodies (axosomatic synapse).
The response of the postsynaptic ending to the neurotransmitter binding results in a change in the postsynaptic cell’s excitability: it will make the postsynaptic cell either more or less likely to fire an action potential. If the number of excitatory postsynaptic events are high enough, they will add to cause an action potential in the postsynaptic cell and a continuation of the “message”.
Many psychoactive drugs and neurotoxins can change the properties of neurotransmitter release, neurotransmitter reuptake and the availability of receptor binding sites.
![]()
Resource 2
Action Potential
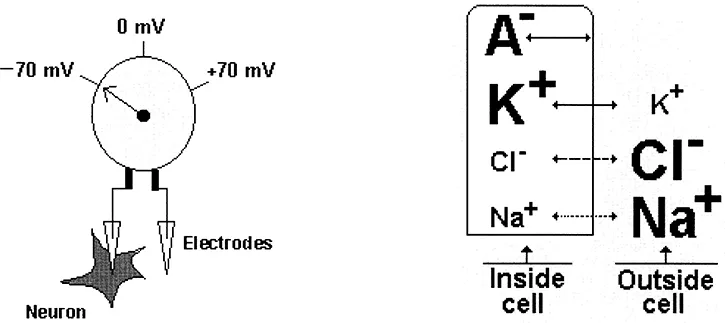
Neurons send messages through an electrochemical process. This means that chemicals result in an electrical signal. Chemicals in the body are “electrically-charged” — when they have an electrical charge, they are called “ions”. The important ions in the nervous system are sodium and potassium (both have 1 positive charge, +), calcium (has 2 positive charges, ++) and chloride (has a negative charge, −). There are also some negatively charged protein molecules. It is also important to remember that nerve cells are surrounded by a membrane that allows some ions to pass through while it blocks the passage of other ions. This type of membrane is called semi-permeable.
Resting Membrane Potential
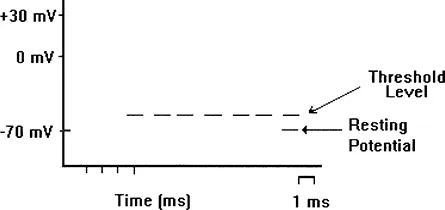
When a neuron is not sending a signal, it is said to be “at rest”. When a neuron is at rest, the inside of the neuron is negative relative to the outside. While the concentrations of the different ions attempt to balance out on both sides of the membrane, they cannot because the cell membrane allows only some ions to pass through channels (ion channels). At rest, potassium ions (K+) can cross through the membrane easily. Also at rest, chloride ions (Cl−)and sodium ions (Na+) have a more difficult time crossing. The negatively charged protein molecules (A−) inside the neuron cannot cross the membrane. In addition to these selective ion channels, there is a pump that uses energy to move 3 sodium ions out of the neuron for every 2 potassium ions it puts in. Finally, when all these forces balance out, and the difference in the voltage between the inside and outside of the neuron is measured, you have the resting potential. The resting membrane potential of a neuron is about −70 mV (mV=millivolt) — this means that the inside of the neuron is 70 mV less than the outside. At rest, there are relatively more sodium ions outside the neuron and more potassium ions inside that neuron.
Action Potential
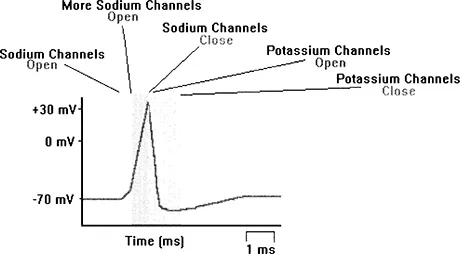
So the resting potential indicates what is happening with the neuron at rest. The action potential indicates what happens when the neuron transmits information from one cell to another. Neuroscientists use other words, such as a “spike” or an “impulse” to describe the action potential. The action potential is an explosion of electrical activity that is created by a depolarizing current. This means that some event (a stimulus) causes the resting potential to move toward 0 mV. When the depolarization reaches about −55 mV a neuron will fire an action potential. This is the threshold. If the neuron does not reach this critical threshold level, then no action potential will fire. Also, when the threshold level is reached, an action potential of a fixed sized will always fire…for any given neuron, the size of the action potential is always the same. There are no big or small action potentials in one nerve cell — all action potentials are the same size. Therefore, the neuron either does not reach the threshold or a complete action potential is fired — this is the “ALL OR NONE” principle.
The “cause” of the action potential is an exchange of ions across the neuron membrane. A stimulus first results in the opening of sodium channels. Since there are a lot more sodium ions on the outside, and the inside of the neuron is negative relative to the outside, sodium ions rush into the neuron. Remember, sodium has a positive charge, so the neuron becomes more positive and becomes depolarized. It takes longer for potassium channels to open. When they do open, potassium rushes out of the cell, reversing the depolarization. Also at about this time, sodium channels start to close. This causes the action potential to go back toward −70 mV (a repolarization). The action potential actually goes past −70 mV (a hyperpolarization) since the potassium channels stay open a bit too long. Gradually, the ion concentrations go back to resting levels and the cell returns to −70 mV.
And there you have it…the Action Potential.
![]()
Resource 3
Management of the individual with pain
Gate Control Theory
In 1965, Melzack and Wall proposed that sensory perception is the result of activation of transmission (T) cells in the dorsal horn of the spinal cord, which in turn results from a balance of peripheral input along large-diameter (A-alpha and A-beta) and small-diameter (A-delta and C) afferent nerve fibers (Fig. 1). Activity from both large and small afferent neurons directly activates the T cell. However, noxious input transmitted via small-diameter fibers also inhibits inhibitory interneurons in the dorsal horn, thus decreasing the effect of presynaptic inhibition on the T cell from the interneurons and ultimately resulting in a net increase in perception of painful input.
In contrast, activity traveling along large-diameter afferent fibers activates the inhibitory interneurons, thus facilitating presynaptic inhibition of the T cell and ultimately resulting in a “closing of the spinal gate,” or a decrease in the perception of sensory activity. In the early 1970s, transcutaneous electrical nerve stimulation (TENS) was viewed as a form of comfortable peripheral sensory input that could decrease pain perception by preferentially increasing the large-diameter afferent fiber input and facilitating presynaptic inhibition of the T cell, thus decreasing conscious pain perception. For instance, TENS has been demonstrated to be effective in relieving pain associated with postherpetic neuralgia, a disease that results in degeneration of large-diameter afferent fibers. Conventional TENS, when applied to the painful region or to a segmentally related region in which the population of large-diameter fibers remains intact, effectively controls the pain associated with postherpetic neuralgia by activating the remaining large-diameter afferent fibers that lie in close proximity to the pathologically active small-diameter afferent neurons in the neuraxis. Other analgesic treatment interventions, including massage or vibration, may also be explained by this theory.
The gate control theory was criticized for failing to 1) account for a variety of painful conditions in which small-diameter afferents were preferentially destroyed and 2) consider the role of higher centers in conscious pain perception. In 1968, Melzack and Casey suggested a modification of the gate control theory to account for activation of higher centers. They added the limbic and reticular systems, both of which are known to affect pain perception, emotional phases of affect, and motor responses. Higher centers in the neocortex also monitor painful afferent input by “comparing” it with past experiences and learned responses. Melzack and Casey suggested that a “central control trigger” activated by input to these higher centers might influence activity in the dorsal horn via descending systems and also might contribute to pain modulation. Thus, a mechanism for pain control via distraction, meditation, or relaxation was elucidated.
Stimulation-Produced Analgesia
A more recent theory of pain modulation is that of stimulation-produced analgesia (SPA), which involves the production and utilization of endogenous opiates, such as endorphins and enkephalins. In 1978, Basbaum and Fields proposed a negative feedback loop mechanism to account for analgesia resulting from low-frequency, high-intensity (acupuncture-like) TENS. They suggested that the noxious input associated with acupuncture-like TENS activates ascending pathways, leading to awareness of pain. Along these pathways, certain axons synapse within medullary reticular formation nuclei. Input from these nuclei then is transmitted to the periaqueductal gray (PAG) regions of the midbrain and thalamus, regions that have high concentrations of endogenous opiates and opiate receptors. When these regions are activated, efferent axons synapse within nuclei in the raphe magnus and reticularis gigantocellularis (RCG). Output from these nuclei descends in the spinal cord and makes enkephalinergic synapses that inhibit spinal transmission of Substance P, which is implicated as a neurotransmitter between axons conveying noxious information. Thus, the application of acupuncture-like TENS may activate a negative feedback loop that ultimately blocks further transmission of noxious information.
Because activation of endorphin-mediated analgesia may be blocked by naloxone, an opiate antagonist, analgesic procedures that are suspected of being endorphin mediated can be identified. Administration of naloxone will reverse this analgesia or return an elevated pain threshold to pretreatment values. Use of low-frequency, high-intensity electrical stimulation of acupuncture points and remote anatomical sites as an endorphin-mediated analgesia has been confirmed by some investigators and denied by others.
Analgesia resulting from acupuncture, acupressure, or cognitive interventions (eg, distraction, imagery, hypnosis) has also been associated with an endorphin-mediated mechanism. As methods of histochemical and electrophysiological data acquisition become more sophisticated, additional neurophysiological mechanisms (as well as confirmation or refutation of current ones) will add to our understanding of pain perception and modulation.
Motivational and Affective Components
Motivational and affective components influence an individual’s perception of and response to pain. Factors that influence a person’s emotional interpretation of and response to pain include age, sex, ethnicity, culture, religious background, attention and distraction levels, environment (eg, who’s watching), and the response of others to his or her behavior. In addition, behavioral responses to pain depend on previous experience with pain, responses learned from others, and perception of control over the cause of the pain.
Acute vs Chronic Pain
Acute pain is often described as pain of less than 6 months duration for which an underlying pathology can be identified. Tissue inflammation, damage, or destruction is often related somatically, or in a referred distribution, to the location and intensity of the person’s pain report. The pain is well localized and defined by the patient. Medication inta...