- 288 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Dr. Wendy Ware, author of the highly acclaimed Cardiovascular Disease in Small Animal Medicine, has brought together specialist contributors to produce this important addition to the Self-Assessment Color Review series.The book presents a wide variety of cases involving cardiothoracic diseases, mainly focusing on the causes of respiratory distress
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
CardiologySelf-Assessment Color Review: Small Animal Cardiopulmonary Medicine
1, 2: Questions
1 A 4-year-old male Rottweiler (1) is presented with a history of a chronic dry cough. Lately he has become anorexic and he now is having trouble breathing. You observe increased respiratory rate and effort. On auscultation you hear no cardiac murmur, but notice increased breath sounds and pulmonary crackles.
i. Describe characteristics of the dog’s appearance that indicate respiratory distress.
ii. How can respiratory pattern help suggest the location of disease in patients with respiratory distress?

2 A 13-year-old neutered male Shih Tzu has been coughing for the past 3 weeks, after he was at a boarding facility for several weeks. Decreased appetite and weight loss were noted recently. Amoxicillin with clavulanate and hydrocodone were prescribed elsewhere for suspected bronchitis, but the owner has had trouble administering the medication. The dog is quiet, but alert and responsive. Body temperature, HR, and respiratory rate are normal. Soft pulmonary crackles are heard over the left hemithorax. Tracheal palpation elicits a non-productive cough. The rest of the physical examination is normal. Chest radiographs show a moderate to severe bronchointerstitial pattern in the caudal lung with alveolar infiltrates in the right cranial lobe. Cardiac size and pulmonary vasculature are normal. A hemogram shows mild thrombocytosis, but is otherwise normal; serum chemistries and urinalysis are unremarkable. Bronchoscopy (2a, b) and BAL are performed.
i. What findings are shown in the bronchoscopic images?
ii. What differential diagnoses should be considered?
iii. How would you proceed with this case?


1, 2: Answers
1 i. His posture suggests severe respiratory distress (‘orthopnea’). Dogs with orthopnea stand or sit with their elbows abducted (allowing full rib expansion) and neck extended, resist lateral or dorsally recumbent positions, and are reluctant to eat and drink or even swallow saliva (note saliva hanging from this dog’s mouth). Dilated pupils also suggest anxiety (note tapetal reflection in photograph).
ii. Respiratory rate and character can provide diagnostic clues. Reduced lung compliance produces a ‘restrictive’ (rapid and shallow) breathing pattern, which minimizes the work of ventilating stiffer lungs. Exhalation or both phases may appear labored. Pulmonary edema, other interstitial infiltrative disease (e.g. bacterial pneumonia, as in this dog), and pulmonary fibrosis produce this pattern; inspiratory pulmonary crackles are common. Partial lung collapse from pleural effusion or other pleural space disease also decreases lung compliance, although large-volume effusion can cause slow, labored inspiration with pronounced abdominal effort.
Airway narrowing causes an ‘obstructive’ breathing pattern. Slower, deeper breaths reduce frictional resistance and respiratory work, although respiratory rate can be normal or increased with peripheral airway disease. The location of the narrowing determines which phase is more labored and (often) prolonged. Lower airway obstruction causes expiratory difficulty, sometimes with wheezing. Upper airway obstruction produces slow or labored inspiration, with or without stridor.
2 i. The airways appear diffusely edematous with mild erythema consistent with generalized bronchial inflammation. Small yellowish tan nodules are seen on some surfaces (2b, from right cranial bronchus).
ii. The radiographic pattern suggests pneumonia or an infiltrative inflammatory or neoplastic disease. Given the history of boarding, infectious tracheobronchitis with secondary pneumonia is a consideration. Small nodules within the airways most often result from chronic inflammation and mucosal proliferation secondary to chronic bronchitis, but neoplastic infiltration is another consideration. Nodules found only near the carina may signal infection with the parasite Oslerus osleri in endemic areas. This dog’s systemic signs, along with the relatively recent onset of coughing, are not typical for chronic bronchitis.
iii. In addition to BAL cytologic analysis and culture, airway brushings and pinch biopsy of a nodule should be obtained during the bronchoscopic procedure. If evaluation of these samples does not yield a definitive diagnosis, lung biopsy is recommended. In this dog, cytologic evaluation revealed mild purulent inflammation, mild chronic hemorrhage, and variably-sized cohesive clusters of highly vacuolated cells thought to be carcinoma cells. BAL cultures yielded no aerobic or anaerobic growth.
3, 4: Questions
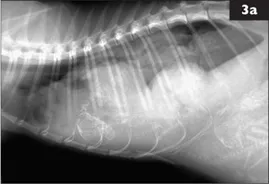

3 A 3-year-old female DSH cat is presented for 1 week of lethargy and increased respiratory effort. She is at 56 days of gestation. A similar episode occurred with the previous pregnancy and responded favorably to antibiotic therapy. This episode seems to be worse. Right lateral (3a) and DV (3b) thoracic radiographs are made.
i. What radiographic abnormalities are evident?
ii. What is the radiographic diagnosis?
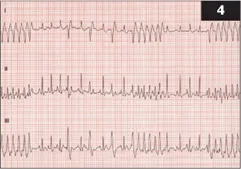
4 A 9-year-old female Dalmation is presented because of a collapse episode earlier in the day. She has been less active lately and becomes winded easily when on walks. The dog appears anxious and slightly tachypneic. Mucous membranes are pink, femoral pulses are weak and of variable intensity, and the HR is rapid and irregular. There is a soft systolic murmur heard best at the right apex, but also heard at the left apex. Lung sounds are increased. You record an ECG. Simultaneous leads I, II, and III at 25 mm/s, 1 cm = 1 mV are shown (4).
i. What is the ECG diagnosis?
ii. How would you initially manage this case?
iii. What do you recommend next?
3, 4: Answers
3 i. There is increased opacity in the ventral and right halves of the thoracic cavity. Only a short dorsal segment of the left crus of the diaphragm is distinct; the remainder is effaced by the increased thoracic opacity. The trachea is displaced dorsally, but remains mid-line in the DV view. The heart is shifted dorsally and to the left. Only the left lung lobes are well inflated with well-defined vessels. The increased thoracic opacity is a mix of solid soft tissue or fluid and mineralized opacity of fetal skeletal structures. A fetal skull is evident ventrally at the 5th intercostal space and a different fetal lumbar spine crosses the pleura-peritoneal junction ventrally.
ii. Right-sided diaphragmatic hernia with thoracic displacement of gravid uterus and probably liver. The degree of fetal skeletal mineralization is consistent with late-term gestation. No signs of fetal death are evident. Ultrasound would be valuable to determine fetal viability. In several reports, the most common organs to be herniated through a tear in the diaphragm are liver, stomach, and small intestine. Several case reports of diaphragmatic herniation of gravid uterus in dogs appear in the literature.
4 i. Paroxysmal ventricular tachycardia (at 300 bpm) is seen at the beginning of the strip, just after the middle, and at the right edge. Sinus tachycardia (at 180 bpm) is evident intermittently. Single ventricular premature complexes also occur, and are easier to distinguish in leads I and III. The sinus complexes indicate a normal mean electrical axis. P waves are slightly wide (0.05 second) consistent with LA enlargement; sinus QRS complexes are also wide (~0.08 second), suggesting myocardial disease and abnormal intraventricular conduction. Other complex measurements are normal. Each 1 mm box = 0.04 second at 25 mm/s.
ii. IV lidocaine is the initial drug of choice for acute treatment of ventricular tachyarrhythmias. An IV catheter is placed as soon as possible. Supplemental O2 may be helpful. The dog should be carried/carted if it must be moved; stress should be minimized.
iii. Identify underlying abnormalities as soon as possible; screen for electrolyte or other metabolic or hematologic abnormalities, obtain thoracic (and possibly abdominal) radiographs, as well as an echocardiogram to assess cardiac structure and function. Additional antiarrhythmic strategies are used if lidocaine is ineffective and for long-term therapy (see Further reading). Additional therapy depends on test results. This dog had dilated cardiomyopathy.
5, 6: Questions
5 The owner of a 12-week-old kitten complains of ‘noisy breathing’. The kitten was adopted 4 weeks ago from the animal shelter and has always made a lot of noise with normal breathing. However, the sound has become more pronounced as the kitten has grown. Breathing is especially noisy when the kitten plays or is excited. Occasionally the kitten gags when eating, but otherwise has been normal. High-pitched...
Table of contents
- Cover Page
- Self-Assessment Color Review: Small Animal Cardiopulmonary Medicine
- Acknowledgements
- Copyright Page
- Preface
- Contributors
- Additional image acknowledgements
- Abbreviations
- Classification of cases
- Contributed cases
- Self-Assessment Color Review: Small Animal Cardiopulmonary Medicine
- Drugs used for cardiac and respiratory diseases
- Further reading
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Small Animal Cardiopulmonary Medicine by Wendy Ware in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.