- 512 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Endothelial Cells in Health and Disease
About this book
This reference serves as the first source to gather current data from endothelial cell biologists in various disciplines to summarize recent progress in the field-providing a complete understanding of the endothelium in health and disease and demonstrating its potential as a therapeutic target.
Information
1
The Endothelium as an Organ
William C.Aird
Department of Medicine, Beth Israel Deaconess Medical Center and Harvard Medical School, Boston, Massachusetts, U.S.A.
1. INTRODUCTION
The endothelium, which lines the blood vessels of the vascular tree, is a truly pervasive cell layer, weighing 1 kg in an average-sized human and covering a total surface area of 4000–7000 m2 (1). Endothelial cells from a single human, when lined end-to-end, would wrap more than four times around the circumference of the earth. The endothelium is not inert, but rather is highly active, participating in several physiological processes, including the control of vasomotor tone, the trafficking of cells and nutrients, the maintenance of blood fluidity, the regulation of permeability, and the formation of new blood vessels (2).
According to the American Heritage Dictionary, an organ is defined as “a differentiated part of an organism, such as an eye, wing, or leaf that performs a specific function.” The Webster’s Revised Unabridged Dictionary defines an organ as a “natural part or structure in an animal or a plant, capable of performing some special action (termed its function), which is essential to the life or well being of the whole.” While the endothelium surely meets these criteria for an organ, it has yet to be widely accepted on these terms. In this chapter, I will argue that its membership into the “organ club” is long overdue.
2. THE BENCH-TO-BEDSIDE DISCONNECT
If one peruses the table of contents and indexes of the more popular medical texts or on-call references, one finds little or no mention of the endothelium. The terms “endothelial cells” and “endothelium” are missing not only from the Merk Manual Index, but also from the 64-page July 2003 index of Scientific American Medicine. In the 15th edition of Harrison’s Principles of Internal Medicine, the index refers only to “endothelial injury, in sclerosis,” and “endothelial cell(s), interactions with lymphocytes; vascular proliferation” (3). In contrast to virtually every other conceivable organ, the endothelium lacks formal representation and organized support, that is, there is no subspecialty training in endothelial biomedicine, nor are there national or international societies for the endothelium. As physicians, few of us are attuned to the health of this cell layer as we interview and examine our patients. Diarrhea, syncope, or jaundice equivalents do not presently exist for the endothelium. There is no “endothelial box” to circle or check off as we move through the review of systems. Moreover, the endothelium is not amenable to the traditional maneuvers of inspection, palpation, percussion, and auscultation. When it comes to laboratory testing, while renal function is readily assayed with urea and creatinine; liver function with transaminases and/or bilirubin; and hematological function with a complete blood count and peripheral smear, there are no convenient and reliable markers for endothelial cell dysfunction.
Table 1 Pub Med References According to Keyword and Yeara
In a recent Pub Med search, the keywords “endothelial cells” and “endothelium” yielded a total of approximately 55,000–85,000 articles, respectively (Table 1); the term “endotheliology,” a total of 1. This of course is no surprise, since current medical lexicon does not include the term “endotheliology” (nor for that matter any analogous term that embraces an endothelial-centric clinical discipline). But that is precisely the point. Contrast the above ratio with that in the liver or heart fields and one begins to see a curious disconnect (Table 1). In other words, despite the exponential growth of (largely basic science) studies over the years, endothelial disease continues to fly well below the clinical “radar screen.” There are several explanations for this bench-to-bedside gap, three of which are discussed below.
2.1. Out of Sight; Out of Mind
One explanation for the under-appreciation of the endothelium as an organ relates to its hidden and enigmatic nature. The endothelium rarely “shows its hand,” at least in the classic ways that we, as physicians, are trained to detect. Like the hematological system, the endothelium is highly diffuse and spatially distributed, extending to all reaches of the human body. Yet unlike blood cells, the endothelial lining is tethered to the blood vessel wall and therefore inaccessible and poorly amenable to study. Although assays do exist for circulating markers of “activated” endothelium, many of these lack specificity, and as single markers provide little in the way of useful information. Pathological specimens of the endothelium are not routinely available and even if they were, the findings would not necessarily correlate with function.
2.2. Historical Legacies
A second factor that has paradoxically contributed to an under-appreciation of the endothelium as an organ relates to the traditional link between vascular biology (and by extension, endothelial cell biology) and cardiology. The connection is steeped in history, its roots dating back to William Harvey’s discovery of the circulation in the early 1600s. Following Harvey’s seminal work, the prevailing view of the cardiovascular system was that of a closed circulatory loop consisting of a pump and series of conduit vessels, with the singular role of delivering oxygen and nutrients to the various tissues of the body. Over the next 400 years, clinical and basic research focused largely on the pump itself, namely on the coronary arteries, the contractile apparatus, the conduction system, and the conduit vessels vis-à-vis their impact on the function of the heart (e.g., hypertension). These developments contributed to and were reinforced by the founding of a large clinical discipline (cardiology), powerful societal infrastructure (American Heart Association), highly successful public awareness campaigns, generous private and public funding, and enormous progress inresearch and development. The importance of these milestones cannot beoverestimated. They have led to vastly improved detection, prevention, andtreatment of coronary artery disease.
Over the past 40 years, however, two seminal observations have revolutionized the field of vascular biology and, when taken together, argue for a more complete synthesis of the field. First was the recognition that the endothelium is not an inert barrier, but rather a highly active cell layer that is involved in a wide variety of homeostatic processes. The second important observation was that the endothelium, in traversing each and every organ, establishes a dialogue that is unique to the underlying tissue—in effect marching to the tune of the local microenvironment. This endothelial-tissue interface plays an important role not only in maintaining health of the organism, but also in dictating the focal nature of vascular disease states. Viewed from this perspective, the study of the endothelium transcends all clinical disciplines. While 20 years ago, one was hard pressed to identify more than a small handful of disorders in which the endothelium played a prominent role, today it may be argued that virtually every disease state involves the endothelium, either as a primary determinant of disease or as a victim of collateral damage (Table 2).
2.3. Complexity
A final consideration that helps explain the bench-to-bedside chasm relates to the complexity of the endothelium. It was not that long ago that many investigators subscribed to the one gene-one enzyme-single function hypothesis. The goal of the human genome project was to develop a blueprint for human health and disease and to establish a menu list for selective drug targeting. One of the surprises arising from this project was a discovery that human genome contains a mere 30,000 genes—compared with an estimated 14,000 genes in Drosophila. These results indicate that complexity does not scale with the number of genes. The discordance is explained in part by differences in alternative splicing and variation in posttranslational modification. More importantly, complexity arises from the connections between components, that is, the regulatory network of protein-protein, protein-RNA, and protein-DNA interactions. Stated another way, all biological systems—including the endothelium—are non-linear and display emergent properties. Most investigators in vascular biology (this author included) tend to focus on specific aspects of endothelial cell function using in vitro assays. In doing so, we may overlook critical levels of organization that are essential to a full understanding of the system (Fig. 1). Just as one could never map the human mind by studying a cultured monolayer of neurons, one cannot rely solely upon in vitro systems to predict and model the behavior of the intact endothelium. An important goal for the future, which will be expanded on below, is to learn how to harness the strength of reductionist and holistic approaches to better understand the algorithms that link individual endothelial cells to blood vessels, blood vessels to organs, and organs to the whole organism.
Table 2 Role of Endothelium in Disease
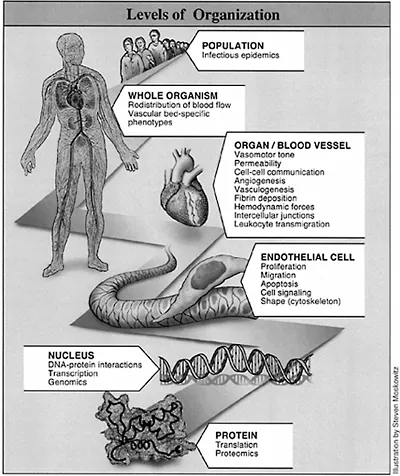
Figure 1 Levels of organization. As with all biological systems, the endothelium displays emergent properties. While each level of organization offers a unique platform for investigation, it is important to recognize that microlevel properties do not necessarily predict for macrobehavior. Indeed, as shown in this schematic, certain properties of the endothelium and vasculature are expressed only at higher levels of organization. Representative examples of level-specific properties are shown.
3. FALLING THROUGH THE CRACKS—A REAL-WORLD EXAMPLE
Let us consider one example of how the conceptual gap in endothelial-based disease has had an impact on patient care. The case study is severe sepsis, defined as systemic inflammatory response to infection with secondary organ failure. Patients with severe sepsis are typically admitted to the intensive care unit. Since the syndrome is complicated by organ dysfunction, medical care is provided not only by critical care physicians but also by a team of organ-specific consultants, including nephrologists, neurologists, hematologists, and cardiologists. The pathophysiology of sepsis is complex and includes a non-linear interplay between multiple cell types and soluble mediators, including components of the inflammatory and coagulation pathway (4) (see Chapter 20). Over the past decade, enormous resources have been expended on sepsis trials, with more than 10,000 patients enrolled in over 20 placebo-controlled, randomized Phase 3 clinical trials. The vast majority of these therapies have failed to improve survival in patients with severe sepsis. A notable exception is a recombinant form of the natural anticoagulant activated protein C (rhAPC), which was shown in the PROWESS study to reduce 28-day all cause mortality in this patient population (5).
The results of the PROWESS trial have created an identity crisis for intensivists and hematologists alike. The critical care field has finally come across an agent that saves lives in severe sepsis. However, the biological plausibility of its mechanism of action is mired in a maze of inflammatory and coagulation pathways. Hematologists have had their own struggles, in this case to make sense of the fact that after 20 years of failed trials in sepsis, the critical care world has embraced a molecule that is near and dear to their hearts as a life-saving measure in a patient population with which they are barely familiar with, and through a mechanism certainly more complicated than simple anticoagulation.
In fact, recent evidence suggests that the common underlying thread in severe sepsis is endothelial cell dysfunction and the efficacy of aPC may ultimately be explained by its attenuation of adverse endothelial cell processes, such as apoptosis (6,7). However, the extent to which this is true will remain unknown as long as the intact endothelium continues to defy diagnostic interrogation.
At a clinical level, an under-appreciation both for the non-linear nature of the host response to infection and the importance of the endothelium as an organ system may have an impact on patient care. In some cases, physicians who lack a full understanding of sepsis pathophysiology, as well as the potential mechanisms of action and risk-benefit profile of rhAPC, may avoid prescribing the agent for fear of the unknown. In other cases, poorly informed clinicians may administer the agent, unprepared for its potential complications. Finally, there exist a growing number of physicians genuinely interested in broadening their understanding of the complexities of the host response, and learning more about the endothelium as a component of this response. Owing to the bench-to-bedside gap in the endothelial field, these individuals currently have limited resources. As long as an understanding of the role of the endothelium eludes ...
Table of contents
- COVER PAGE
- TITLE PAGE
- COPYRIGHT PAGE
- FOREWORD
- PREFACE
- CONTRIBUTORS
- 1: THE ENDOTHELIUM AS AN ORGAN
- 2: BLOOD-BRAIN BARRIER
- 3: LYMPHATIC ENDOTHELIUM
- 4: HIGH ENDOTHELIAL VENULES
- 5: THE USE OF PROTEOMICS TO MAP PHENOTYPIC HETEROGENEITY OF THE ENDOTHELIUM
- 6: THE USE OF GENOMICS TO MAP PHENOTYPIC HETEROGENEITY OF THE ENDOTHELIUM
- 7: THE ROLE OF GENETIC PREDETERMINANTS IN REGULATING THE PHENOTYPIC HETEROGENEITY OF THE ENDOTHELIUM
- 8: THE USE OF FATE MAPPING STUDIES TO FOLLOW LINEAGE DETERMINATION OF THE ENDOTHELIUM
- 9: OXYGEN REGULATION OF ENDOTHELIAL CELL PHENOTYPES
- 10: FLUID MECHANICAL FORCES AS EXTRINSIC MODIFIERS OF ENDOTHELIAL FUNCTION
- 11: VASCULAR BED-SPECIFIC SIGNALING AND ANGIOGENESIS
- 12: DIFFERENTIAL REGULATION OF ENDOTHELIAL CELL BARRIER FUNCTION
- 13: DIFFERENTIAL REGULATION OF LEUKOCYTE-ENDOTHELIAL CELL INTERACTIONS
- 14: VASCULAR BIOLOGY OF THE PLACENTA
- 15: BLOOD ENDOTHELIAL CELLS
- 16: DETERMINATION OF ENDOTHELIAL HETEROGENEITY BY THE RECRUITMENT OF BONE MARROW DERIVED ENDOTHELIAL PROGENITORS
- 17: TRANSCRIPTIONAL NETWORKS AND ENDOTHELIAL LINEAGE
- 18: THE DIVERSITY OF VASCULAR DISEASE: A CLINICIAN’S PERSPECTIVE
- 19: MOLECULAR TARGETS OF TUMOR VASCULATURE
- 20: THE ROLE OF THE ENDOTHELIUM IN SEVERE SEPSIS AND MULTIPLE ORGAN DYSFUNCTION
- 21: THE HEPATIC SINUSOIDAL ENDOTHELIAL CELL AS A PRIMARY TARGET OF DISEASE
- 22: ENDOTHELIUM AND HEMOSTASIS
- 23: THROMBOTIC MICROANGIOPATHIES: ROLE OF MICROVASCULAR ENDOTHELIUM IN PATHOGENESIS
- 24: PULMONARY CIRCULATION AND PULMONARY HYPERTENSION
- 25: ENDOTHELIAL CELL PHENOTYPES ASSOCIATED WITH ORGAN TRANSPLANTATION
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Endothelial Cells in Health and Disease by William C. Aird in PDF and/or ePUB format, as well as other popular books in Biological Sciences & Hematology. We have over 1.5 million books available in our catalogue for you to explore.