Assessment and Treatment of Non-Suicidal Self-Injury: A Clinical Perspective is the ideal primer for anyone who works with people who self-injure. Profiling who is affected as well as what their behaviour includes, the book explores the range of factors behind why people self-injure, from the influence of social media to the need for self-regulation, and offers recommendations for both assessment and outpatient treatment.
Throughout, the book is permeated by profound respect for those who use self-injury in an attempt to live a good life, while conveying a deep understanding of the challenges that self-injury presents for family members and treatment professionals. It recognizes that the behaviour can spread in hospital wards or other institutional setting, introducing the concept of self-injury by proxy, and assesses the range of therapies available, including CBT, MBT, ERGT and family therapy. Each chapter is complemented by clinical vignettes.
In an era when a great number of professionals will come into contact with someone who self-injures – including teachers, social workers and nurses as well as therapists – The Assessment and Treatment of Non-Suicidal Self-Injury is an invaluable resource that examines both the causes and the treatments available.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Although this book also addresses other forms of self-injury, its main focus is on non-suicidal self-injury (NSSI) as defined by the International Society for the Study of Self-Injury (ISSS) in 2007:
Socially unacceptable, intentional, and direct injuring of one’s own body tissue without suicidal intent.
In this definition, ‘direct’ implies that the act has immediate physical consequences, such as the wounds resulting from cutting. The definition thus excludes indirect self-injury, which refers to a behaviour that may eventually result in physical injury, such as eating disorders, overdosing on medicine, substance abuse, smoking or other behaviours where the injury results from chemical processes within the body.
The self-injury has to be deliberate and ‘intentional’, in contrast to behaviour that accidentally results in injury to oneself. The definition also specifies that the injury has to affect ‘body tissue’, although the degree may vary from superficial scratches or bruising to more severe damage, for example as a result of cutting. The act has to be ‘socially unacceptable’; this excludes self-injurious behaviour that is more or less culturally sanctioned, such as self-inflicted piercings, tattoos and body modifications and rites of passage that are not addressed here (Favazza, 1996).
The focus in the present book is on acts that defy or deviate from cultural norms and values. However, normalcy and deviation are fluid, contextually defined concepts, and in certain youth subcultures, for example, cutting is socially accepted and more or less a part of the group identity (Young et al., 2014).
Finally, the act of self-injury, under this definition, is not driven by a desire or an intention to commit suicide. If someone cuts their arm with the desire to open an artery in order to bleed to death, that is, naturally, a form of self-injury, but as it must be categorized as attempted suicide it falls outside the definition of self-injury that is applied in the present book.
Direct self-injury
Direct self-injury means that the self-inflicted injury is immediately apparent, for example, in the form of a wound, bleeding, bruising, a scratch or other signs on the skin. The following are the most prevalent methods for NSSI:
Cutting
Cutting may be done with a variety of sharp implements, such as a razor, a knife, a shard of glass or anything else that is sharp enough to penetrate the skin, such as a broken CD or a credit card snapped in two. Numerous studies have identified cutting as the most common method for NSSI (e.g., Victor et al., 2018). Klonsky (2007) notes that 50–90% of persons who engage in NSSI do so by cutting. Other studies have found that 20–30% keep the wound open by picking at it, thus delaying the healing process (Bresin & Schoenleber, 2015), and that some increase the sensation of pain by pouring salt or acidic substances into the wound.
Cutting may be directed at any part of the body, although some parts are more commonly chosen than others. The most commonly endorsed body locations in a 2018 survey (Victor et al., 2018) were arms (88%), followed by legs (60%) and abdomen/stomach (31%); males were more likely to report cutting on their torso/ chest. Laukkanen et al. (2013) found that two-thirds of self-cutting adolescents reported only cutting the upper arms, while a third also cut other parts of the body. Cutting on other parts of body than the arms was more common among females and associated with a wide range of emotional and dissociative symptoms and suicidal ideation. Some cut in straight lines or carved words, while others engaged in less structured self-injury by hacking at or even removing parts of the tissue.
A woman who habitually made superficial cuts in her skin had attempted to block out violent flashbacks by making deep cuts to her arm that eventually ruined the tendons in her lower arm.
Patients who cut their genitals, breasts or face are directing their self-injury against parts of the body that are more emotionally charged, in both positive and negative ways. These patients are typically more severely psychologically affected than those who merely make superficial cuts in, for example, their arms or legs. The genitals may be associated with emotions such as pleasure, joy and pride, but also with shame, guilt or anxiety, perhaps as a result of sexual abuse. A study (Møhl & Rubæk, submitted) found a significant link between having been subjected to sexual abuse during childhood and later developing genital self-injury.
Some cut impulsively in connection with stressful experiences (‘triggers’), but many plan the behaviour and wait until conditions are right. They may need to be alone, to avoid being interrupted or discovered; they may plan around what they are going to do afterwards; or they may put off cutting in order to ‘have something to look forward to’. Some have even described that they derive pleasure from anticipating the release that comes with cutting. One patient described taking steps to make sure she would not be disturbed and interrupted while cutting. She prepared for the act by getting cotton, plaster and disinfectant ready and regarded these preparations as an almost pleasurable part of the process (Stacy et al., 2018).
The duration of planning and delaying the act of cutting can vary from hours to days or even weeks. One 17-year-old woman described how she had promised her parents to avoid cutting during their three-week holiday, and she managed to keep her promise despite cutting almost daily, sometimes several times daily, as they got close to the departure date. Knowing that she could resume cutting when she returned home was a relief and something for her to look forward to. After returning home she had several severe incidents with NSSI.
Hitting
Hitting oneself with a fist or various objects is the second-most-frequent form of NSSI, mentioned by about one-third of people who self-injure (Bresin & Schoenleber, 2015). A Danish study of NSSI among upper-secondary school students found that 47% of the respondent who self-injured had done so by hitting themselves. Respectively, 64% of the males and 39% of the females who self-injured had done so by hitting themselves (Møhl & Skandsen, 2012). Hitting may also involve, for example, punching a wall or a doorjamb, which may result in bone fractures or other serious injury.
Scratching
Scratching till the blood flows is another frequently used method. In a study among American college students, Whitlock et al. (2006) identified scratching as the most common form of self-injury, and a meta-analysis found that between 21% (males) and 31% (females) who had self-injured had used scratching (Bresin & Schoenleber, 2015).
Burning
Burning oneself with a cigarette or a lighter or by pouring boiling water or coffee over a hand, for example, is a method that is used by 15–35% of people who self-injure (Klonsky, 2007). The result is a painful burn with a high risk of infection. Bresin and Schoenleber (2015) found that 20% of the males and 18% of the females who had self-injured had burned themselves.
Compulsive headbanging
Headbanging, where the person repeatedly bangs their head against a wall, can result in thickened areas in the forehead and temple region and intracranial bleeding. Some report that they mainly engage in headbanging when they are bored, while others do it when they are under stress. A meta-analysis found that head-banging occurs in 28% of males and 24% of females (Bresin & Schoenleber, 2015), but it is more prevalent among individuals with intellectual disabilities or neuropsychiatric conditions, such as Tourette’s or Lesch-Nyhan syndrome, where it may serve as a form of auto-stimulation.
Trichotillomania
Hair pulling is an independent diagnosis (trichotillomania) in ICD-10, categorized under Impulse Disorders (F63.3), and in the DSM-5, where it is categorized under OCD (312.39). The condition is characterized by considerable hair loss due to the irresistible, recurring urge to pull out one’s own hair. Hair pulling may be directed at the scalp, eye brows or pubic region and often has an automatic character, as a form of distraction, but it may also occur in response to anxiety or stress. It may result in large bald spots. Bresin and Schoenleber (2015) report that 12% of males and 35% of females report pulling hair.
Skin picking
Skin picking, which is another independent diagnosis categorized under OCD in DSM-5 (698.4) (Excoriation Skin Picking Disorder), consists in pulling off skin, either in flakes or by searching for and attempting to remove skin irregularities or impurities; the behaviour may result in severe skin irritation and infections with scabs that the person can maintain by picking at them. These patients often consult dermatologists without coming into contact with psychiatric care. Lifetime prevalence for skin picking is 1.4%, and the disorder is more common among women.
In the novel Cat’s Eye (1989, p. 113) the Canadian writer Margaret Atwood describes how a young girl self-injures, in part through skin picking, in connection with being bullied by a group of girls from her school:
‘In the endless time when Cordelia had such power over me, I peeled the skin off my feet. I did it at night, when I was supposed to be sleeping. My feet would be cool and slightly damp, like the skin of mushrooms. I would begin with the big toes. I would bend my foot up and bite a small opening in the thickest part of the skin on the bottom, along the outside edge. Then, with my finger nails, which I never bit because why bite something that didn’t hurt, I would pull the skin off in narrow strips. I would do the same to the other big toe, then to the ball of each foot the heel of each. I would go down as far as the blood. Nobody but me ever looked at my feet, so nobody knew that I was doing it. In the mornings I would pull my socks on, over my peeled feet. It was painful to walk but not impossible. The pain gave me something definite to think about, something immediate. It was something to hold on to’.
Self-inflicted fractures
Rarer methods include self-inflicted fractures or the practice of swallowing objects (such as lighters, teaspoons, hairpins, scissors) that later have to be removed surgically. These practices may be found among psychotic patients or, for example, patients who are incarcerated.
Other methods
As many as 80% of people who regularly self-injure use a variety of methods, often depending on the circumstances and on the specific emotions they are dealing with (Gratz, 2001). For example, a young woman began to hit herself in the face and burn herself with cigarettes or a lighter while she was hospitalized and hence prevented from cutting. For her own protection, the staff had placed all sharp objects out of reach and kept her under constant watch.
Another young woman reported that she would cut herself almost daily, but that she burned herself with a cigarette when she was in severe distress: ‘A cigarette hurts more than cutting, and it lasts longer. You can feel it for a long time. That’s good when I feel really, really bad. That’s why I do it’. None of these methods are really life-threatening unless they are taken to the extreme, which they rarely are by people who self-injure regularly.
Other methods for direct NSSI include biting (16% of the males and 27% of the females); inserting needles or similar objects under the skin (20% of the males and 24% of the females); carving the skin (18% of the males and 27% of the females); sewing the skin with thread; rubbing the skin violently using a rubber eraser to cause burns; pouring acid on the skin; or self-inflicted tattoos (Bresin & Schoenleber, 2015).
Indirect self-injury
Indirect self-injury can be defined as an act that does not lead directly to an injury but instead results in increased risk of an unintended long-term consequence. With indirect self-injury such as heavy drinking or smoking, the actual harm stemming from the behaviour is unclear, and in many cases the harmful effects are a matter of chance. Some people can consume large quantities of alcohol over several years without suffering major long-term effects. Although the habit increases their risk of liver damage, they may still be lucky enough to avoid it. This is an important difference compared to direct self-injury, where the damage is predictable and occurs as an immediate result of the behaviour. Unlike direct self-injury, it can be difficult to define indirect self-injury precisely, except as a behaviour that increases the risk of developing health issues.
Examples of indirect self-injuring behaviour
Eating disorders, either starving oneself or overeating
Substance abuse
Unsafe sex
Reckless driving
Getting into fights
Gambling
Indirect self-injury falls outside the definition that is applied in the present book. It is mentioned here because it often correlates with direct self-injury. Many people who self-injure, for example by cutting, do so while they are under the influence of alcohol or drugs, which lowers the threshold for direct self-injury. A Danish study of self-injury among upper-secondary school students found that 53.9% had experience with one or more types of indirect self-injury defined as 1) alcohol-related blackout, 2) binge eating and purging and/or deliberately starving themselves and 3) use of harder drugs (for example amphetamine, LSD, heroin). We also found a correlation between direct and indirect self-injury in the group overall. Among the male respondents, the correlation was twice as high as it was among the female participants. Thus, direct self-injury implies an elevated risk of indirect self-injury in the form of drug use, alcohol-related blackouts or eating disorders (Møhl et al., 2014). A study (Claes et al., 2015) found that 59% of patients with an eating disorder engaged in at least one type of NSSI (most frequently cutting), with no significant difference in rates of NSSI among eating disorder subtypes.
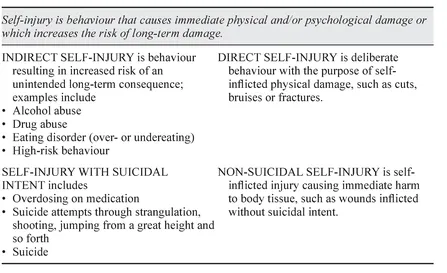
Table 1.1 Overview of different forms of self-injury.
In a comparison of indirect and direct NSSI, Germain and Hooley (2012) found that individuals who engage in direct self-injury are more critical of themselves and more like...
Table of contents
Cover
Half Title
Title
Copyright
Contents
List of illustrations
Introduction
1 What is non-suicidal self-injury?
2 Non-suicidal self-injury - an autonomous diagnosis?
3 Epidemiology and gender differences
4 Self-injury as a sign of the times?
5 Historical theories and new models for understanding non-suicidal self-injury
6 Attachment, affect regulation and growing up in an invalidating environment
7 From meaning to function
8 Pathophysiology and neurobiological perspectives on self-injury
9 Assessment of patients with non-suicidal self-injury
10 Treatment of non-suicidal self-injury - an overview
11 Dialectical Behaviour Therapy
12 Mentalization-Based Therapy - keeping mind in mind
13 Treating self-injury during hospitalization
14 When a loved one self-injures
References
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Assessment and Treatment of Non-Suicidal Self-Injury by Bo Møhl in PDF and/or ePUB format, as well as other popular books in Psychology & History & Theory in Psychology. We have over 1.5 million books available in our catalogue for you to explore.