- 256 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
This new volume in the established and well-respected series of Self-Assessment Color Reviews covers all aspects of adult emergency medicine. Some 250 cases are presented randomly to reflect real-life practice. Each case consists of one or more questions, illustrated by stimulating visual material including clinical photographs, imaging and electro
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
Medicine1, 2: Questions
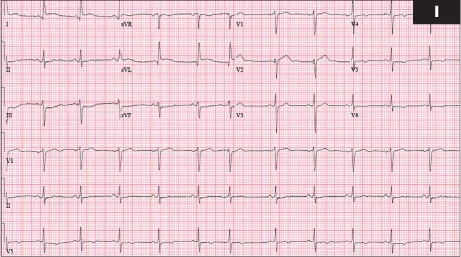
1 A 49-year-old male had diabetes mellitus and known hyperlipidemia. He presented with 2 hours of severe precordial chest pain, shortness of breath, and nausea. He appeared ill and was very diaphoretic.
i. What does this ECG suggest (1)?
ii. What are indications for reperfusion therapy?

2 A 34-year-old male sustained this injury when he twisted his ankle while running (2).
i. What is the diagnosis?
ii. What associated complications are likely, and how should they be managed?
1, 2: Answers
1 i. The ECG demonstrates normal sinus rhythm at about 70 bpm (premature atrial contraction in sixth beat). ST segments are elevated over 1 mm in lateral leads (I and aVL), with slight reciprocal ST depression in inferior leads III and aVF. T waves are inverted in leads V4 to V6. This is consistent with acute lateral wall myocardial infarction. Cardiac catheterization revealed acute LAD coronary artery occlusion.
ii. Rapid and aggressive management of acute myocardial infarction greatly reduces morbidity and mortality. New ST elevation of 1 mm or more in contiguous associated leads, in the setting of chest pain or anginal equivalents of recent onset (usually <6 hours from symptom onset, but even longer if stuttering course or ongoing ischemia), mandates reperfusion therapy. Associated leads are as follows: inferior leads: II, III, and aVF; lateral leads: I, aVL, V5, and V6; anterior leads: V1 to V4; posterior leads: V7 to V9; right ventricular leads: right-sided V1 to V6 (particularly right V4). ECG changes for posterior wall myocardial infarction are seen indirectly in anterior precordial leads, with tall R waves in V1 to V3 with ST segment depression and upright T waves. New onset of left bundle branch block with suspected ongoing ischemia is also an indication for reperfusion therapy. Serial ECGs, and comparison to previous ones, is often helpful in borderline cases.
2 i. This is an open medial ankle injury, usually due to an eversion and external rotation mechanism. Associated deltoid ligament injury or medial malleolus avulsion is likely, and a spiral distal fibular fracture is usually present. Rarely, deltoid ligament or medial malleolus injuries are associated with a tear in the tibiofibular syndesmosis, often with a proximal fibular fracture. This is termed a Maisonneuve fracture and may lead to chronic ankle instability if not recognized and managed correctly. Occasionally, an open ankle can occur without fracture, particularly with penetrating trauma. Careful neurovascular examination is important. Simple radiographs are usually adequate to assess for fracture, with CT reserved for complex fractures.
ii. Liberal analgesia is indicated. Neurovascular status may be compromised by dislocation, in which case prompt reduction is indicated. Open fractures should be covered by wet sterile dressings. Broad-spectrum antibiotics and tetanus prophylaxis are indicated. Early orthopedic consultation is important since joint irrigation, exploration, and surgical repair are necessary.
3, 4: Questions
3 A 32-year-old male presented 30 minutes after being an unrestrained passenger in a motor vehicle collision. He was talking, but a bit combative. BP was 80/54 mmHg (10.7/7.2 kPa) and P 156 bpm. He had clear lungs, a stable pelvis, no extremity injuries, and no evidence of significant external bleeding. He had moderate left upper quadrant pain.
i. What is the appropriate evaluation and management of this patient?
ii. Discuss some of the controversies in management?
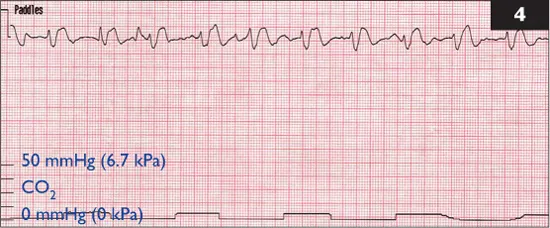
4 A 72-year-old female was intubated after cardiac arrest and had not recovered a pulse despite aggressive attempts at CPR.
i. What does her respiratory CO2 waveform capnogram tell you (4)?
ii. Should CPR be continued?
3, 4: Answers
3 i. Because of probable hemorrhagic shock, evaluation and management must be concomitant and expeditious. The patient appears to have a stable airway. IV access with two large caliber catheters should be obtained and crystalloid infused rapidly to improve perfusion. Laboratory tests include CBC along with type and cross-matching for packed RBCs. Chest and pelvis radiographs should be obtained. Ultrasound FAST techniques should look at the heart, hepatorenal, splenorenal, and bladder spaces to screen for intra-abdominal trauma. CT of the abdomen and pelvis is an alternative evaluation technique, but may cause dangerous delay if hemodynamic instability exists. Peritoneal lavage to evaluate for significant intra-abdominal bleeding has largely been supplanted by the above methods. Immediate surgical consultation is indicated. Decisions for operative intervention are often made clinically if evidence of significant intra-abdominal injury and/or hemodynamic instability exists. Packed RBCs should be infused if hypoperfusion persists after about 2 liters of crystalloid.
ii. Submaximal volume resuscitation to avoid increased bleeding may improve survival if rapid surgical intervention, with minimal IV fluids, is done quickly to repair bleeding intra-abdominal organs. Selective arterial embolization for bleeding hepatic and/or splenic injuries is used in some clinical settings. Nonoperative management of splenic or hepatic injuries is frequent when hemodynamic stabilization can be accomplished. However, fear of unrecognized associated intra-abdominal injuries and resultant complications makes nonoperative management controversial.
4 i. The monitor strip reveals an irregular wide-complex rhythm, which in this setting represents pulseless electrical activity. The capnographic waveform demonstrates an appropriate but small rise to about 8 mmHg (1.1 kPa) in CO2 with exhalation, with return to zero during inhalation. This confirms appropriate endotracheal tube placement in the airway. However, the low expiratory CO2 level in this setting suggests that minimal blood is being delivered to the lungs for ventilatory exchange. This confirms severe hypoperfusion to the brain, heart, and other organs as well, suggesting that CPR is inadequate. Sudden improvement in expiratory CO2 levels with CPR suggests improved perfusion, but elevations may also occur with sodium bicarbonate administration, which can cause confusion if not understood.
ii. Attempts to improve CPR by more aggressive chest compression or other techniques should be considered. If expiratory CO2 remains <10 mmHg (1.3 kPa) for more than a few minutes, continued efforts are likely to be futile.
5, 6: Questions

5 This 20-year-old male presented with a painful mouth, along with frequent bleeding from his gums over the past few days (5).
i. What is this problem, and what are the predisposing factors?
ii. How should it be treated?

6 This 25-year-old patient had several days of severe sore throat with fever, diffuse myalgias, and increased fatigue (6). His streptococcal throat screen was negative.
i. What are the diagnostic considerations here?
ii. Is any therapy likely to help?
5, 6: Answers
5 i. Acute necrotizing ulcerative gingivostomatitis (ANUG), also known as Vincent’s angina or trench mouth. It was prevalent among soldiers stuck in the trenches during World War I. ANUG is a progressive, painful anterior mouth infection with swelling, ulceration, and gum necrosis. It may progress to involve the entire mouth and throat as well as cause dental loss. ANUG is typically caused by overgrowth of normal oral bacteria, including Bacteroides, Fusobacterium, and other anaerobic species. Factors such as poor oral hygiene, inadequate nutrition, stress, and other infections predispose to trench mouth. It has become increasingly common with AIDS. The patient presents with painful, swollen gums along with bad breath and foul taste. The gums are often hyperemic, with a gray film and ulcers between the teeth, and bleed with any irritation.
ii. Treatment begins with improved oral hygiene, using dilute hydrogen peroxide or saltwater rinses. Penicillin remains the antibiotic therapy of choice, although metronidazole is also used. Smoking cessation, proper nutrition, and improved dental care help with prevention. HIV testing may be indicated.
6 i. This is acute pharyngitis, usually due to various viral infections (adenovirus most commonly, but Epstein–Barr and HIV also important). Bacterial causes are mostly streptococcal, but Corynebacterium diphtheriae, Neisseria gonorrheae, Chlamydia, and Mycoplasma are other considerations. Recently, overgrowth of Fusobacterium necrophorum, a normal oral flora, has been implicated in formation of peritonsillar abscesses and/or Lemierre’s syndrome (infectious thrombophlebitis of the internal jugular vein). Candida albicans and chemical irritants are other common etiologies. Throat pain, fever, difficulty swallowing, and headache are frequent with acute pharyngitis, along with various rashes and lymphadenopathy. Various antigen assays for Streptococcus may be useful, but false negatives related mainly to collection techniques and false positives due to chronic carrier state may occur. The global burden of rheumatic heart disease complicating streptococcal disease is found disproportionally in developing countries. Testing for infectious mononucleosis by a heterophile antibody test may be negative early, as sensitivity peaks at 2–6 weeks. CBC may show a suggestive increase in total lymphocytes to >60%, with atypical lymphocytes >10%. Primary HIV infection may cause a mononucleosis-like illness and should be considered in at-risk patients, with quantitative HIV-1 RNA viral load by PCR positive as early as 11 days after infection.
ii. Paracetamol and/or NSAIDs may provide effective pain relief. Penicillin remains the antibiotic of choice for streptococcal pharyngitis and reduces risk of developing rheumatic fever. Clindamycin is effective if the patient is penicillin allergic. Oral corticosteroids, particularly single-dose dexamethasone, reduce severity and duration of symptoms.
7, 8: Questions

7 A 43-year-old female fell off a ladder and had severe pain in her left heel.
i. What does this radiograph demonstrate (7)?
ii. Is surgery necessary?

8 A 27-year-old male presented after being found unconscious outside someone’s home. BP was 96/60 mmHg (12.8/8.0 kPa), P ...
Table of contents
- Cover Page
- Self-Assessment Color Review: Adult Emergency Medicine
- Acknowledgements
- Copyright Page
- Preface
- Classification of cases
- Abbreviations
- Self-Assessment Color Review: Adult Emergency Medicine
- Further reading
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Adult Emergency Medicine by John O'Brien in PDF and/or ePUB format, as well as other popular books in Medicine & Emergency Medicine & Critical Care. We have over 1.5 million books available in our catalogue for you to explore.