Architecture and Health recognizes the built environment and health as inextricable encouraging a new mind-set for the profession. Over 40 international award-winning projects are included to explore innovative design principles linked to health outcomes. The book is organized into three interdependent health domains—individual, community, and global—in which each case study proposes context-specific architectural responses. Case studies include children's hospitals, rehabilitation facilities, elderly housing, mental health facilities, cancer support centers, clinics, healthy communities, healthcare campuses, wellness centers, healing gardens, commercial offices, infrastructure for developing countries, sustainable design, and more. Representing the United States, Africa, Asia, Europe, and Australia, each author brings a new perspective to health and its related architectural response.
This book brings a timely focus to a subject matter commonly constricted by normative building practices and transforms the dialogue into one of creativity and innovation. With over 200 color images, this book is an essential read for architects, designers, and students to explore and analyze designed environments that promote health and well-being.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Architecture and other design disciplines have long lagged behind in driving the social, political, financial, and environmental arguments for creating spaces that promote health and healing. Discoveries in modern medicine, presumably because of their emphasis on measurable outcomes, have ushered in the dominance of the hard sciences over design and the definition of health. After decades, centuries, and even millennia of partial understandings of what health is, we are finally beginning to expand its definition to include well-being, a noticeable shift from an emphasis on “sickness” to “wellness”. With the myriad of testing possibilities and big data available to the twenty-first century, and evolved understandings of healthcare practice, architecture can regain agency in its interactions with health in all forms. Accompanying this opportunity is the expectation that the built environment cannot be a passive actor in contributing to the improvement of health. This reinstatement of responsibility warrants new design responses that address a broader view of health, encompassing physical, psychological, emotional, social, and environmental influences.
The purpose of this book is to provide a way forward for those who are interested in understanding how the built environment is connected to this broader view of health. To illustrate this concept, a collection of case studies has been compiled to show how to plan and design environments that contribute to the health of individuals, organizations and communities, and larger natural ecosystems. Each case study explores the intersection of design and health for a diverse range of building types, scales, and contexts.
1.2Influence of the Built Environment on Health
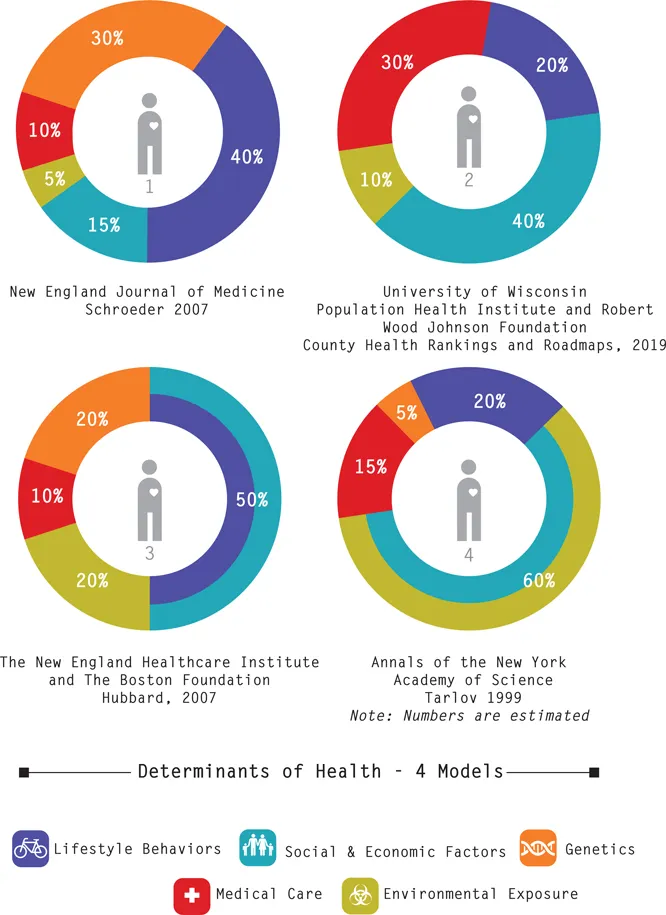
Studies and public discourse centered on longevity (one of the most cited indicators of health) accurately identify it as the sum of an individual’s lifestyle, social context, and more (Buettner 2012). Undoubtedly, factors relating to diet, physical activity, genetics, and access to medicine and technology affect health outcomes. But, as suggested in the seminal paper “We Can Do Better—Improving the Health of the American People”, pathways to better health outcomes do not generally depend on better medical care (Schroeder 2007). In fact, the major determinants of health extend far beyond the provision of organized healthcare services, which themselves ironically have been estimated to account for only 10% of health outcomes. By comparison, the largest share contributing to health outcomes is attributed to individual behaviors (40%) and secondly, to social and environmental factors (20%) (McGinnis et al. 2002; Schroeder 2007). When we consider that individual behaviors rely partially on what the social environment affords, it becomes evident that the built environment’s contribution to health, insofar as it shapes lifestyle, is highly significant. A comparison of four commonly referenced models that quantify health outcomes as a result of five different determinants shows that between 55% and 80% of overall health is driven by lifestyle behaviors and social/economic factors; between 5% and 20% is driven by environmental exposure, between 10% and 30% is driven by access to healthcare services; and between 10% and 30% is driven by genetics (Figure 1.1).
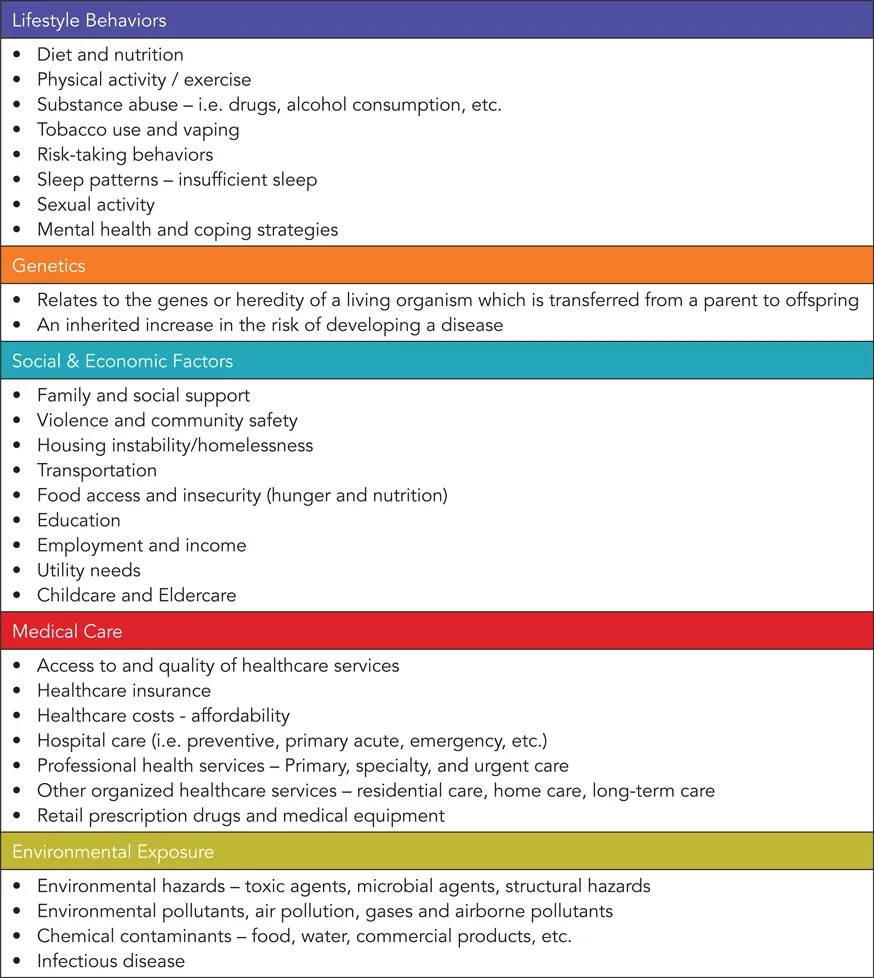
While the four different models break down health into five determinants, it is not always clear what constitutes each determinant. To help understand these further, a list of factors that commonly align with each is presented in Figure 1.2.
The influence of the built environment on health is vast, yet it is frequently subjugated to other concerns. Of course, healthcare services are essential for treating and curing the sick and will persist. However, it is imperative to broaden our perspective and recognize that biological, social, economic, and environmental factors—and their interrelationships—all contribute to health. Social services, public health programs, and environmental infrastructure, like quality housing, schools, daycare, parks, and even sidewalks and bike lanes, are necessary complements to organized healthcare facilities. A broader perspective of health means we need to think about how to design physical environments in conjunction with programs and services, recognizing that healthcare isn’t provided in just one specific setting.
1.3Healthcare Spending: An Impetus for Change
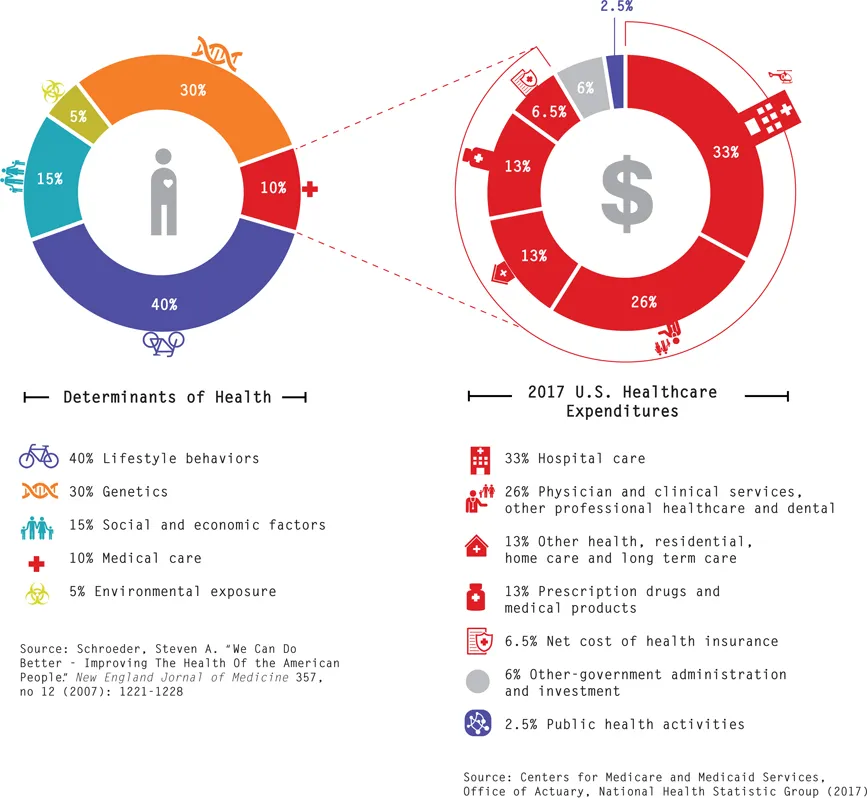
According to the Centers for Medicare and Medicaid Services, the U.S. channeled 53% of its annual healthcare budget in 2018 to hospital care, and physician and clinical services (Figure 1.3). By comparison, the government spent less than 3% of the healthcare budget on matters pertaining to public health, significantly less than the 10% spent on retail prescription drugs. When you look at spending patterns in relation to health determinants, the misallocation of resources is clear. While we put 3% of our healthcare budget toward the chunk of healthcare determinants that account for 60% of health outcomes, we put 53% of these resources toward organized healthcare services that account for only 10% of health outcomes.
▸ Figure 1.1
Determinants of health.
Source: Dina Battisto and Eva Henrich
The U.S. spends nearly $10,750 a year on healthcare for each American, accounting for almost 18% of the total gross domestic product (GDP) in 2017 (CMS.gov). Even though the U.S. spends twice the amount compared to other countries on healthcare, we continue to lag on health indicators, such as mortality and life expectancy (OECD). While this huge investment in organized health-care services reduces mortality rates in the U.S., preventative diseases, such as congestive heart failure, asthma, hypertension, and type II diabetes, are on the
▸ Figure 1.2
Factors that contribute to the five determinants of health.
Source: Dina Battisto
rise. Moreover, costly chronic conditions are the largest contributors to high hospital admission rates. Many of these preventative diseases are chronic, lasting a lifetime, and are closely tied to individual behaviors and social factors. These preventative diseases, and the costs associated with treating them, could be curbed with health promotion efforts and better designed environments.
▴ Figure 1.3
U.S. healthcare spending in relation to health determinants.
Source: Dina Battisto and Eva Henrich
In tandem with health status, well-being is the root of a person’s happiness. According to the World Happiness Report, which is a global ranking of happiness levels across 156 countries, the United States is not even in the top ten. As of 2019 the U.S. ranks nineteenth and has continued to drop in rankings over the last two years. Jeffrey Sachs, Columbia University professor and director of the Center for Sustainable Development, provides an explanation claiming “America’s subjective well-being is being systematically undermined by three interrelated epidemic diseases, notably obesity, substance abuse (especially opioid addiction), and depression” (Sachs 2018, p. 147). When you look at the top-ranking countries, like Finland, Denmark, Switzerland, and Canada, you see they perform noticeably well in six key variables: “income (GDP per capita), healthy life expectancy, social support, freedom, trust (absence of corruption), and generosity” (Helliwell, Layard, and Sachs 2019, p. 22). Five of these six variables address dimensions of health beyond organized medical care. Clearly, we in the U.S. are missing something.
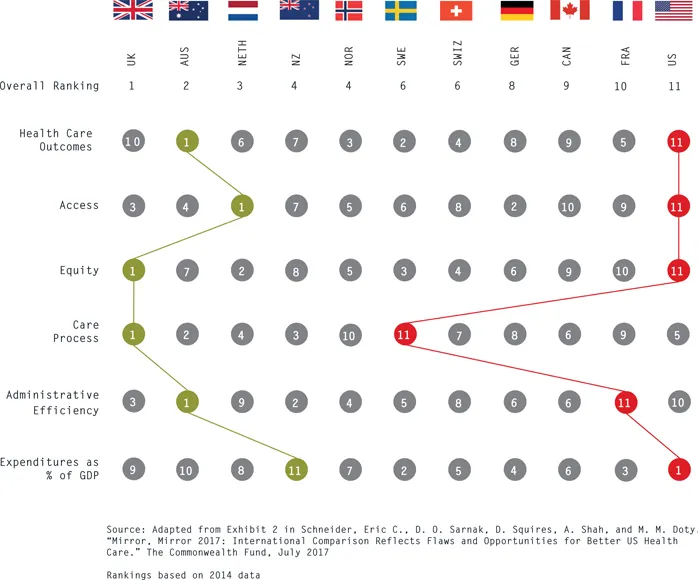
▴ Figure 1.4
Healthcare system performance rankings.
Source: Dina Battisto and Eva Henrich
1.4Models of Health and Their Architectural Response: A Brief Retrospective
An examination of the past helps reveal how we’ve veered so far off course in pinpointing a formula for better health outcomes. Different eras have addressed
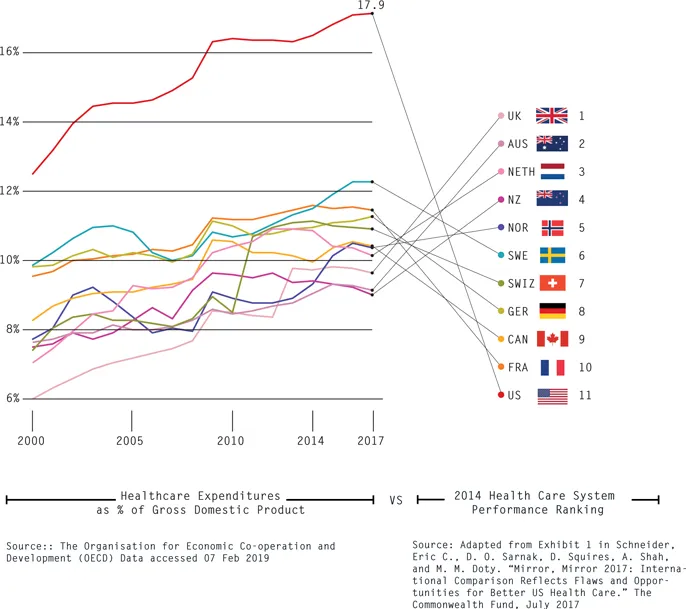
▸ Figure 1.5
Healthcare spending as a percentage of GDP, 1980–2014.
Source: Dina Battisto and Eva Henrich
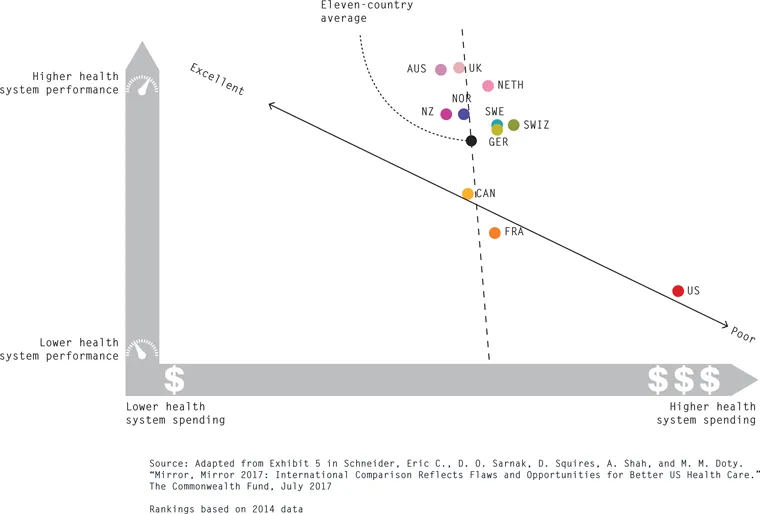
▸ Figure 1.6
Performance of 11 different healthcare systems in relation to spending.
Source: Dina Battisto and Eva Henrich
health in unique ways, using architecture to varying degrees and effectiveness. Within the beliefs and motivations of a given era, a model of health describes the method in which health services are delivered. Models of health, whether salutogenic or pathogenic in nature, lead to architectural responses that serve as precedent in improving the health and welfare of populations.
◂ Figure 1.7
World happiness rankings, 2019.
Source: Dina Battisto and Eva Henrich
1.4.1 Salutogenesis: Ancient Civilizations and Civic Wellness
All timelines tracking a focused and concerted effort to care for the needs of humans begin with ayurvedic approaches, recognized today as healthcare. Some historians have traced what is considered to be the first deliberate creation of space for the purpose of caring for individuals as existing through the ayurvedic tradition (Rannan-Eliya and De Mel 1997). Chinese medicine, evolving in Asia some centuries later, combined similar uses of herbs and rituals to balance the body, and likewise was passed along through tradition and scattered practices.
While many of these ancient systems are today largely considered pseudoscientific and at best among the protosciences, it is important to note the emphasis they all had on a holistic view of health that included physical, social, mental, and spiritual health. Greek cities, like Epidaurus, included a mix of wellness-oriented programs in therapeutic surroundings: a library for intellectual pursuits, a theater for entertainment and social interactions, a gymnasium for exercise and fitness, and healing temples for connecting to the gods. In all cases, a clear link is made between health and architecture: healing occurs in places of spiritual sanctity as well as in daily life, whether that be in monumental sanctuaries or socially active baths and markets (Thompson and Goldin 1975).
These approaches to health are closely tied to salutogenesis, a concept later defined by the sociologist Aaron Antonovsky in ...
Table of contents
Cover
Half Title
Title
Copyright
Contents
Foreword
Acknowledgments
Key Terms
1. Introduction: Discovering an Architecture for Health
Part 1 Individual Health
Part 2 Community Health
Part 3 Global Health
About the Editors
List of Contributors
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Architecture and Health by Dina Battisto, Jacob J. Wilhelm, Dina Battisto,Jacob J. Wilhelm in PDF and/or ePUB format, as well as other popular books in Architecture & Architecture General. We have over 1.5 million books available in our catalogue for you to explore.