As the practice of value-based care gains wide adoption, billions of dollars of government and insurer payments are contingent on quality reporting to demonstrate delivery of evidence-based care. Electronic health record (EHR) systems today provide increasing levels of clinical decision support and are the fulcrum for change at the heart of value-based healthcare delivery. In this context, we define applied population health as the use of the EHR system to identify patient cohorts in need of evidence-based interventions, and facilitate actions to address care gaps. The use of registries in the EHR has been transformative in the sense that we can identify and track groups of patients by diagnosis, treatment, enhanced demographics, and administrative relationships and efficiently drive appropriate action at the individual or group level. This is key to achieving economies of scale and delivering timely preventative care to keep patients well and prevent or slow their advance across the secondary and tertiary illness trajectory. The registries are not an end in themselves, but drive a population health engine that operationalizes clinical protocols, the “who, what, and when” of healthcare. The registry engine will drive the gears of standardized processes and workflows to deliver high-value care that reduces variance and waste. These will serve as foundational components to the future evolution of integrated digital health, precision medicine, and ever more sophisticated decision support.
Combining the people, process, and technology to deliver value-based care has proven to be a monumental effort. Pivoting from traditional fee-for-service to value-based care has the promise to more effectively avert poor healthcare outcomes and improve quality of life. This transformation of care delivery at a national scale pledges to keep people healthier through the judicious practice of evidence-based care and optimal deployment of limited clinical resources. Roots of this dissemination blossomed as a result of “value” visioning from key leaders such as Donald Berwick, who asserted that the triple aim of improved population health, improved patient experience, and reduced cost was not only possible but necessary. Subsequently, the recognition that doctors and healthcare workers were facing increasing challenges with the usability of EHR systems and meeting the new quality measurement practices resulted in a fourth aim: improved caregiver experience.(1) It takes just a single human story to move past the statistics and bring home the realities of provider burnout. A young primary care doctor recently shared this email:
I receive 75–100 messages per day from or about my patients. It takes me about 5 minutes to respond to a message. This generates 6.5 to 8.3 hours per day of un-billable work amounting to a full workday for a normal person. The EHR trainer said that he has not seen anyone work faster; he could not even keep up with me. I am also seeing patients, writing notes, and reviewing charts.
As a result of this much work, I sit in a chair and work every waking hour that I am not physically at work. This includes every weekend and every holiday. I have not stopped working long enough to eat food with my family or even open Christmas presents (it is now February). My daughter told me last week, “It is like you are an imaginary mommy.” Being an imaginary person is lonely and unhealthy. As a resident, I worked a lot. I also had good friends, I did yoga, played with my kids, and volunteered as class parent. I was able to take good care of my patients and enjoy being a mother. I never got close to burning out. After 3 months under the load I described, I am completely burned out. This burden of work on physicians demands sacrifices in the quality of patient care, in physician health, and in the well-being of our children. This amount of work prevents me from doing the things I care about most: being an excellent doctor, a healthy person, and loving parent.
—Imaginary Mommy, MD
Bending the curve on the healthcare quality–to–expenditure ratio, however, is recognized to require a fundamental “re-engineering” of healthcare delivery to support the practice of medicine and avert the unintended consequences faced by the “imaginary mommy.”(2) The mere conversion of paper-based processes to electronic form is insufficient to achieve the quadruple aim. We need to vision, design, and shape enterprise-wide systems to thoughtfully direct and improve the efficiency and effectiveness of care delivery. Through the lens of our national healthcare system, financial opportunities and challenges are shaping the practice of applied population health as providers and patients experience it today. This handbook is designed to help large, complex health systems move the needle on quality measures and outcomes while preserving the dignity of patients and providers and the very important moments when they come together for healing and comfort. The primary audience for this book includes both clinical and nonclinical professionals with experience in healthcare delivery. Graduate students will gain a practical understanding of the professional roles engaged in this field to inform their career paths in medicine, nursing, allied health, healthcare administration, public health, clinical informatics, data analytics, or operations research with an emphasis in healthcare. As individuals coalesce into effective teams for population health care delivery, health systems will experience improved patient care, quality measure performance, and revenue from incentives and risk-based contracts.
The book is presented in three parts: 1) Fundamentals 2) Effective Delivery of Applied Population Health, and 3) Applied Population Health Today and Tomorrow, so that the reader may more easily find the material that complements their background and interests.
Part 1: Fundamentals
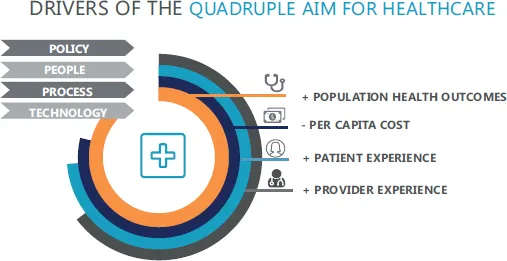
Value-based care seeks to achieve a quadruple aim of improving health outcomes and patient and caregiver experience, while concurrently reducing per capita cost. Policy, people, process, and technology are drivers of market-based healthcare reform to meet these challenges (Figure 1.1). Part 1 provides the reader with the background and common vocabulary that are prerequisite to understanding the effective delivery of applied population health presented in Part 2. We also believe that a shared lexicon of informatics terms will enable multidisciplinary teams to work together more effectively and productively to advance the overall state of practice.
Figure 1.1Drivers of the quadruple aim for healthcare.
Highlights of Part 1 include:
| Policy | A brief history of the U.S. policies driving value-based payment models
Quality measure use in pay-for-performance and risk sharing programs
Value-based measurement framework |
| People | Organizational characteristics
Stepping stones to value-based care
Value improvement governance structure
Patient empanelment and attribution to define doctor–patient relationships |
| | Understanding patients and patient groups
Social determinants of health
New standards for race, ethnicity, and language (REAL)
Data collection for sexual orientation and gender identity (SO/GI) |
| Process | Sample population health protocol
Technology flaws underlying healthcare waste |
| Technology | Introduction to the role of registries in value-based care delivery
Taxonomy and ontology of health registries |
| Measuring the quadruple aims | Population health outcomes
Per capita cost
Patient experience
Provider experience |
| Case studies | Provider engagement practices
Collection of ethnic background data
Doing the right thing with medication monitoring
Use of Social Security decedent data in EHR registry |
Part 2: Effective Delivery of Applied Population Health
When we formed the enterprise population health team in the information services department four years ago, we considered actionable registries in the EHR to be our prime deliverable followed by actionable clinical decision support. However, we grew frustrated with the difficulty of quantifying value with that approach. We had long lead-times for development of registries with large numbers of metrics, and there were disconnects between the registry build, quality measures, and clinical decision support. Gradually, we came to realize that applied population health methods are more effective when rolled out in the following order:
- Identify the quality measure(s) to target for change
- Build the registry with data elements needed for the measure calculations
- Add clinical decision support and supporting workflows to drive performance
- Build real-time dashboards for continuous process measurement
Highlights of Part 2 include:
| Conceptual model | Applied population health technical foundation |
| Prototype system | Do-it-yourself quality measure management |
| Registry design principles | Transitioning from quality measures to registries |
Second-generation
clinical decision support | EHR tools that use the registry engine to drive care |
| Analytics dashboards | Innovative application of dashboards to:
Track rolling performance measures in real time (365 day lookback)
Demonstrate utilization and value of technology
Co-locate quadruple aim outcomes |
Along the way we’ll include case studies to introduce readers to insights and tools for organizing and monitoring quality measure performance. “Field Report” highlights briefly encapsulate challenges and solutions based on our own experience. Exercises and discussion questions encourage individuals and/or small groups to develop innovative solutions. We encourage our readers to wrestle with these scenarios for a deeper understanding of the nuances in quality improvement projects and how each team member contribu...