eBook - ePub
100 Cases in Clinical Pharmacology, Therapeutics and Prescribing
- 226 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
100 Cases in Clinical Pharmacology, Therapeutics and Prescribing
About this book
100 Cases in Clinical Pharmacology, Therapeutics and Prescribing explores scenarios commonly seen by medical students and junior doctors in the ward, emergency department, outpatient clinic or in general practice in which an understanding of pharmacology and sound prescribing practice is central to successful clinical management and safe patient care. A succinct summary of the patient's history, examination and any initial investigations is followed by questions on the diagnosis and management of the case. The answer includes a detailed discussion on each topic, providing practical advice on how to deal with the challenges that occur when prescribing, including planning, drug calculations, prescription review and adverse drug reactions. The book will be invaluable during clinical placements and is an ideal companion during preparation for the Prescribing Safety Assessment
examination.
Making speedy and appropriate clinical decisions, and choosing the best course of action to take as a result, is one of the most important and challenging parts of training to become a doctor. These true-to-life cases will teach students and junior doctors to prescribe appropriately, and to hone their diagnostic and management skills.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Clinical MedicineSECTION 1
BASIC PRINCIPLES
CASE 1: THE CYTOCHROME P450 SYSTEM
History
A 54-year-old female patient presented to the emergency department with a 6-h history of worsening shortness of breath and sharp, right-sided chest pain that was worse on deep inspiration. She denied experiencing palpitations, did not complain of nausea, and was not feeling lightheaded.
She had a history of recurrent deep vein thromboses for which she was on lifelong warfarin. Her INR had been stable at 3.0–3.5 with 5 mg warfarin once daily for more than a year and had last been checked 4 weeks ago. Her only other past medical history was a recent diagnosis of active pulmonary tuberculosis, for which the patient had been prescribed isoniazid (alongside pyridoxine), rifampicin, pyrazinamide and ethambutol.
The patient worked as a primary school teacher and was usually fit and well. She had never smoked and denied any regular alcohol intake. There was no relevant family history.
Examination
The patient appeared moderately dyspnoeic on exertion but was able to speak comfortably at rest. Her pulse rate was 110 beats per minute and regular and her blood pressure was stable at 130/84 mmHg. Her respiratory rate was 22 breaths per minute. She was afebrile.
Results
Blood test | Result | Reference range |
White cell count | 7.8 × 109/L | 4.0–11.0 ×109/L |
Haemoglobin | 123 g/L | 120–160 g/L |
Platelet count | 400 × 109/L | 150–400 ×109/L |
INR (international normalised ratio) | 1.2 units | 0.8–1.2 units |
A CT pulmonary angiogram scan showed large volume, bilateral pulmonary emboli but no evidence of associated right heart strain.
Questions
1. What is the most likely reason for the patient developing a pulmonary embolus at this point in time?
2. How may this have been prevented?
ANSWERS
1. Although novel oral anti-coagulants are increasingly prescribed for many thromboembolic conditions, warfarin remains one of the more commonly prescribed therapies in complex disease.
The hepatic cytochrome P450 (CYP) system consists of a family of isoenzymes that are involved in the metabolism of many drugs, including warfarin. The rate of drug metabolism is affected by a large number of substances, including other medications and dietary sources that can induce or inhibit the activity of the isoenzymes. Table 1.1 shows a selection of substrates that are affected by inducers and inhibitors of the CYP pathways.
In this instance, the patient has recently commenced treatment with the antibiotic rifampicin, which is a potent inducer of inducer of CYP2C19 – one of the isoenzymes responsible for warfarin metabolism. As the activity of this CYP isoenzyme increases, warfarin is metabolised at a faster rate and may thus reach subtherapeutic levels, which happened in this case and the patient has subsequently developed pulmonary emboli.
2. Warfarin has a narrow therapeutic index, which means that a minor change in dose can cause the drug level to reach sub therapeutic or toxic levels. Warfarin acts by inhibiting vitamin K-dependent synthesis of clotting factors and the INR is used as a measure of the effectiveness of the drug in affecting the prothrombin time.
In situations where potential CYP inducers or inhibitors are introduced, warfarin therapy must be closely monitored. INR measurements will need to be performed more frequently to allow dose adjustments of warfarin as required, until a point is reached where the patient remains stable on the current therapies. As it can take several days to achieve a therapeutic level of warfarin, an additional agent (typically heparin) will initially need to be prescribed for this patient to ensure that she is adequately anti-coagulated.
Hepatic enzyme inhibition | Hepatic enzyme induction | |||
|---|---|---|---|---|
Enzyme inhibitors | Drugs with effects potentiated by inhibitors: | Enzyme inducers | Drugs with effects impaired by inducers: | |
Allopurinol | Carbamazepine | Barbiturates | Hydrocortisone | |
Cimetidine | Ciclosporin | Carbamazepine | Oral contraceptive pill | |
Ciprofloxacin | Phenytoin | Ethanol (chronic misuse) | Phenytoin | |
Disulfiram | Theophyllines | Phenytoin | Warfarin | |
Erythromycin | Warfarin | Rifampicin | ||
Ethanol (acute intoxication) | Sulphonylureas | |||
Isoniazid | ||||
Omeprazole | ||||
Sodium valproate | ||||
Sulphonamides | ||||
 | Key Points |
|---|---|
| 1. The CYP system is a family of isoenzymes that are responsible for the metabolism of many drugs. 2. Enzyme inducers will lead to rapid metabolism of certain drugs and may impair their effects. 3. Enzyme inhibitors will reduce the rate of metabolism of certain drugs and thus increase their effects. | |
CASE 2: THERAPEUTIC LEVELS
History
An 85-year-old lady was admitted from a nursing home to the emergency department complaining of worsening shortness of breath and a sensation that her heart was ‘racing’. She denied symptoms of chest pain and cough and reported feeling well over recent weeks aside from intermittent episodes of palpitations. Her past medical history included hypertension, ischaemic heart disease and heart failure, as well as a previous episode of atrial fibrillation when she had a community-acquired pneumonia last year. Her regular medications were ramipril 10 mg OD, bendroflumethiazide 2.5 mg OD and digoxin 125 μg OD.
Examination
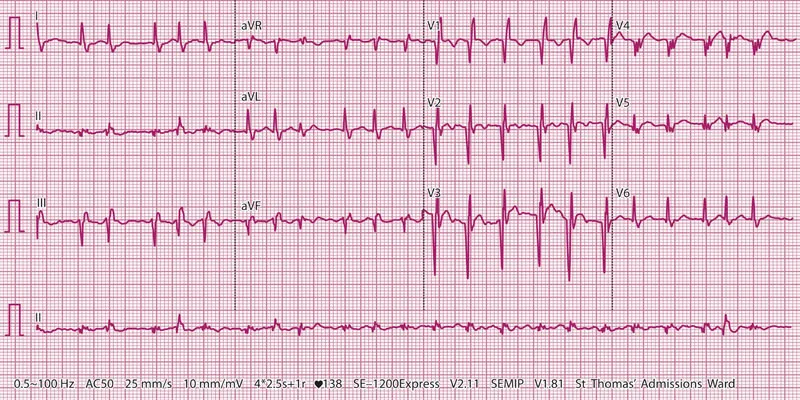
The patient was afebrile and looked comfortable at rest. Her pulse rate was 140 beats per minute and the blood pressure was 104/70 mmHg. The heart sounds were difficult to hear clearly due to the rapid rate; her pulse was noted to be irregularly irregular. There was mild, pitting oedema to the ankles but her jugular venous pressure was not elevated. Her chest was clear, with oxygen saturations of 97% on room air.
Results
The chest X-ray showed clear lung fields. Her ECG is shown below.
Questions
1. What would be the next drug of choice for the acute management...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Preface
- Authors
- Abbreviations
- Reference Ranges for Common Investigations
- Section 1: Basic Principles
- Section 2: Therapeutics
- Section 3: Prescribing Cases
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access 100 Cases in Clinical Pharmacology, Therapeutics and Prescribing by Kerry Layne,Albert Ferro in PDF and/or ePUB format, as well as other popular books in Medicine & Clinical Medicine. We have over 1.5 million books available in our catalogue for you to explore.