eBook - ePub
Catheter-Related Infections
- 648 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Catheter-Related Infections
About this book
This updated reference describes the latest and most effective strategies in the diagnosis, management, and treatment of catheter-related infections (CRIs). The guide describes the pathogenesis of infectious complications while discussing procedures in infection control, catheter and catheter-site care, and patient monitoring and evaluation. This n
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
1
Epidemiology and Impact of Infections Associated with the Use of Intravascular Devices
Philippe Eggimann
Medical Intensive Care Unit Department of Internal Medicine University of Geneva Hospitals Geneva, Switzerland
Didier Pittet
Infection Control Program Department of Internal Medicine University of Geneva Hospitals Geneva, Switzerland
INTRODUCTION
Nosocomial infections are a leading cause of morbidity and mortality among hospitalized patients. They should not, however, be considered as an inevitable tribute to pay to the continuous progress in medicine, considering in particular the sophisticated diagnostic and management strategies applied to the care of complex diseases. The extent of the problem was recently highlighted in the general medical literature in the late 1990s, following a publication by the Institute of Medicine in Washington, DC. In brief, this report estimated that preventable adverse events in the United States, including nosocomial infections, were responsible for 44,000 to 98,000 deaths annually and represent a cost of $17 to $29 billion (1). Mostly based on extrapolation from two studies only, this report has generated a considerable debate in the scientific community (2–9). Comparable data were published in the United Kingdom by the House of Commons in November 2000 (10). This official government report estimated that at least 100,000 infections are acquired in hospitals in England each year. These infections may be responsible for at least 5,000 deaths annually, with cost estimates as high as $1.8 billion (11).
Nosocomial infections now concern 5% to 15% of hospitalized patients and can lead to complications in 25% to 50% of those admitted to intensive care units (ICUs) (12,13). Globally, urinary tract and surgical site infections are the most frequent infections, followed by respiratory and bloodstream infections (14) (Fig. 1). Most data concerning the epidemiology of these infections concern particular types of infections in specialized wards, and general information is sparse. However, it has been repeatedly shown that intravascular devices are among the most significant risk factors for the development of nosocomial infections (15–18).
More precise epidemiological data are available for critically ill patients and those admitted to ICUs, in particular. Among these patients, pneumonia related to mechanical ventilation, intra-abdominal infections following trauma or surgery, and bacteremia or sepsis associated with the use of intravascular devices account for more than 80% of ICU-acquired infections (19,20) (Table 1).
Bloodstream infections represented 12% of all nosocomial infections reported in 10,038 patients from 1417 ICUs in the European Prevalence of Infection in Intensive Care (EPIC) study (15). The National Nosocomial Infection Surveillance (NNIS) system, which took into account only data from ICUs, reported that most nosocomial bloodstream infections are associated with the use of intravascular access, with rates substantially higher among patients with central venous catheters (CVCs) than among those with peripheral lines (19,20).
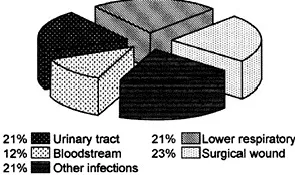
Figure 1 Proportion of nosocomial infections (n=472) occurring among 4252 patients from 18 large Swiss general hospitals in 1999. Data adapted from the 2nd Swiss National Prevalence Study (14).
Table 1 Epidemiology of Leading Nosocomial Infections in Various Types of ICUs in the 1990s
Table 2 Definitions of Infections Associated with the Use of Intravascular Devicesa
DEFINITIONS
One should recognize the difference between definitions used for surveillance purposes and clinical definitions. The surveillance definitions for catheterassociated bloodstream infections include all primary bloodstream infections in patients with an intravascular catheter when other sites of infection have been excluded. The clinical definitions for catheter-related infections include colonization of the device, skin exit-site infection, and microbiologically proven intravascular device-related bloodstream infection (21–27) (Table 2). Microbiological criteria remain a matter of debate among experts, and this issue will be discussed in detail in Chapter 3 of this book. However, the absence of a gold-standard reference technique may provide an explanation for the large difference in the published rates of infections. Accordingly, the clinical definition of catheter-related infections may underestimate the true rate of infections related to intravascular devices.
Important issues must be taken into consideration prior to any discussion of the epidemiology and impact of infections associated with the use of intravascular devices. According to the data regularly reported by the NNIS system, more than 85% of primary bacteremia are considered catheter-associated (28–31). The concept of bloodstream infection used includes not only primary bacteremia, but also clinical sepsis (21,32). This may overestimate the rate of infections related to intravascular devices, but it is probably more representative of the clinical reality and allows comparison of rates in surveillance studies. Although included in some reports, secondary bacteremia—by definition— should not be considered as catheter-related; it is related to another documented focus of infection.
Last but not least, infection rates usually vary according to the type of surveillance performed. In trials or studies designed to study complications associated with the use of intravascular devices, infection rates are frequently higher than in those reporting results for the surveillance of all nosocomial infections. In studies dedicated to catheter surveillance, systematic microbiological investigation might allow expression of infection rates or sites rarely investigated in overall surveys.
Finally, other caveats for surveillance and rate-reporting that may affect infection rates will not be considered in this chapter.
EPIDEMIOLOGY
Infections associated with the use of intravascular devices represent 10% to 20% of all nosocomial infections. Accordingly, they may complicate the hospital stay of 0.5% to 3% of patients admitted in ICUs, and of 3.5% to 10% of those hospitalized in general wards. In the United States, it is estimated that up to 150 million intravascular devices are inserted annually in hospitalized patients, and that 200,000 to 400,000 nosocomial bloodstream infections may occur each year (19,33).
According to the variety of definitions used in the literature, infection rates may be difficult to compare. These rates are also largely influenced by patient case-mix and the purpose of the use of vascular access (34). In this chapter, we focus on the epidemiology and impact of infections associated with the use of intravascular devices in acutely ill patients requiring short-term catheterization. The epidemiology of particular types of devices, such as long-term catheterization for hemodialysis or parenteral nutrition, and surgically implanted devices in immunocompromised patients, will be discussed elsewhere in the book.
The prevalence of bloodstream infections associated with the use of intravascular devices in selected studies performed in critically ill patients varies according to the type of disinfection used for the preparation of the skin before the insertion of a central venous catheter. Studies have repeatedly shown that chlorhexidine-based solutions, although not widely used since the early 1990s, may be more potent than those using povidone-iodine (35–42) (Table 3).
The proportion of catheter-related bloodstream infection may also be extracted from studies exploring the potential effect of antimicrobial-coated intravascular devices, mostly conducted during the second part of the 1990s. In these studies, the prevalence of catheter colonization and of catheter-related bloodstream infections ranged from 5.8% to 71.4% and from 0.3% to 11.0%, respectively (43–60) (Table 4).
Table 3 Rates of Colonization and Catheter-Related Bloodstream Infection According to Type of Disinfectant Used for Cleansing Skin Insertion Site in Selected Series of Critically Ill Patients
Table 4 Rates of Colonization and Catheter-Related Bloodstream Infection Associated with Antiseptic/Antibiotic-Impregnated and Nonimpregnated Central Venous Lines in Selected Series of Critically Ill Patients
Comparisons between infection rates in different types of ICUs are more accurate when infections are reported as incidence-densities related to central venous catheterization days. According to this method, widely diffused by the NNIS system, they range between 2.3 and 16.8 episodes per 1000 catheter-days. Table 5 presents comparisons of selected reports from various types of ICUs (20,28–32,40,58,61–76).
The epidemiology of clinical sepsis is not well established. It accounts for fewer than 3% of all episodes of catheter-related infections reported to the NNIS system (28). The term clinical sepsis is included in the surveillance definitions for primary bloodstream infections published by the CDC to accommodate sepsis episodes where there is no pathogen cultured from blood, and as a complement to the definition of laboratory-confirmed primary bloodstream infection. This entity, which should be used for epidemiological purposes, is, however, relatively close to the definition of the syndromes of systematic inflammatory response, severe sepsis, and septic shock in response to an inflammatory or infectious process (77). At present, only few epidemiological data are available, and the impact of clinical sepsis remains to be determined (42,66,67,78–81) (Table 6).
IMPACT
Several studies have determined the impact of infections associated with the use of intravascular devices on patient morbidity and hospital costs in ICUs. A significant correlation was found between the prevalence rate of ICU-acquired infection and the mortality rate. In the EPIC study, laboratory-proven bloodstream infection, pneumonia, and clinical sepsis were independently associated with increased mortality (15).
The impact of infection is determined by the attributable part of the parameters that are considered. Accordingly, the attributable mortality of nosocomial infections is defined as the difference in the death rate of infected patients and noninfected patients in a series adjusted for the presence of other confounding factors. Several epidemiological methods may be used to determine the attributable mortality, or any other parameter associated with the acquisition of nosocomial infection. Direct estimation is a simple method in which an experienced clinician subjectively estimates if the death of a patient is related to the infection or not. This technique systematically underestimates the attributable part of the mortality. Appropriateness of evaluation protocol is another direct method that is used to estimate the prolongation of the length of stay possibly associated with the infection. Based on standardized criteria, the patient is evaluated daily to determine whether the stay in hospital is related to the underlying disease, a complication resulting from comorbidity or medical care, and/or to the presence of a nosocomial infection.
Table 5 Catheter-Associated Bloodstream Infection Rates in Selected Series of Critically Ill Patients
Table 6 Epidemiology of Different Types of Infections Associated with the Use of Intravascular Devices: Selected Series, Critically Ill Patients
Another method compares two groups of patients: those with and those without a specified nosocomial infection. Differences are expected to be attributable to the nosocomial infection. However, this technique does not take into consideration potential confounding parameters that may exist between the two groups of patients. This effect can be attenuated by including factors potentially related to death or other outcome measures in multivariate analysis...
Table of contents
- COVER PAGE
- TITLE PAGE
- COPYRIGHT PAGE
- INFECTIOUS DISEASE AND THERAPY
- PREFACE
- CONTRIBUTORS
- 1: EPIDEMIOLOGY AND IMPACT OF INFECTIONS ASSOCIATED WITH THE USE OF INTRAVASCULAR DEVICES
- 2: PATHOGENESIS OF VASCULAR CATHETER INFECTIONS
- 3: DIAGNOSIS OF CATHETER-RELATED INFECTIONS
- 4: MANAGEMENT OF INTRAVASCULAR CATHETER-RELATED INFECTIONS
- 5: PREVENTION AND CONTROL OF CATHETER-RELATED INFECTIONS
- 6: CATHETER-RELATED STAPHYLOCOCCUS AUREUS INFECTION
- 7: CATHETER-RELATED INFECTIONS CAUSED BY COAGULASE-NEGATIVE STAPHYLOCOCCI
- 8: INTRAVASCULAR CATHETER-RELATED INFECTIONS DUE TO GRAM-NEGATIVE BACILLI
- 9: FUNGAL INFECTIONS OF CATHETERS
- 10: MISCELLANEOUS ORGANISMS
- 11: CENTRAL-VENOUS CATHETERS
- 12: PERIPHERAL VENOUS CATHETERS
- 13: INFECTIOUS COMPLICATIONS OF PA PULMONARY ARTERY CATHETERS, CORDIS INTRODUCERS, AND PERIPHERAL ARTERIAL CATHETERS
- 14: LONG-TERM CENTRAL VENOUS CATHETERS
- 15: INFECTIONS ASSOCIATED WITH CENTRAL NERVOUS SYSTEM IMPLANTS
- 16: INFECTIONS ASSOCIATED WITH CHRONIC PERITONEAL DIALYSIS
- 17: INFECTIONS ASSOCIATED WITH HEMODIALYSIS VASCULAR ACCESSES AND WITH CATHETERS USED FOR HEMODIALYSIS
- 18: CATHETER-RELATED INFECTIONS IN PEDIATRIC PATIENTS
- 19: INFECTIONS ASSOCIATED WITH URINARY CATHETERS
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Catheter-Related Infections by Harald Seifert, Bernd Jansen, Barry Farr, Harald Seifert,Bernd Jansen,Barry Farr in PDF and/or ePUB format, as well as other popular books in Medicine & Epidemiology. We have over 1.5 million books available in our catalogue for you to explore.