- 240 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Practical Laryngology
About this book
Practical Laryngology is an invaluable guide to laryngology. It covers all the relevant areas in the field, from basic science to disorders and diseases to in-clinic procedures and the future of laryngology. In an easy-to-read format, the book discusses a wide variety of topics including neurological diseases of the larynx, swallowing disorders, la
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
CHAPTER 1
Basic science
Vocal tract anatomy
Gross anatomy
The larynx is located along the midline of the anterior part of the neck, at approximately the level of the third to sixth cervical vertebrae. It extends from the base of the tongue to the trachea, and communicates posteriorly with the oropharynx and the hypopharynx.1
The larynx is subdivided into the supraglottis, glottis and subglottis (Figure 1.1). These subdivisions are most relevant in laryngeal neoplasms, as tumours in different anatomical locations behave differently. The boundary between the supraglottis and glottis is widely accepted to be a horizontal line through the apex of the laryngeal ventricle. In contrast, the transition from the glottis to the subglottis is more controversial. Various authors demarcate the transition at 10 mm below the medial free edge of the vocal fold or 10 mm below the apex of the laryngeal ventricle.2
Laryngeal inlet
The laryngeal inlet is the opening that connects the larynx to the pharynx. Its borders are the epiglottis anteriorly and superiorly, the aryepiglottic folds laterally and the mucosa overlying the arytenoid cartilages and the interarytenoid area posteriorly. The hypopharynx extends laterally to the laryngeal inlet to form the piriform sinuses.
Vestibular folds
The vestibular folds, or the false vocal cords, are bilateral mucosal folds extending from the inner surface of the thyroid cartilage anteriorly to the body of the arytenoid cartilage posteriorly. The body of the vestibular fold is made by the vestibular ligament, the thickened free inferior margin of the quadrangular membrane. The latter is a connective tissue layer extending from the lateral aspect of the epiglottis to the arytenoids. The vestibular folds contain variable muscle structures, which are believed to contribute to their limited movement.3,4
Laryngeal ventricles
The laryngeal ventricles are the spaces between the vestibular and vocal folds and are present bilaterally. They extend anteriorly into the saccule, a tubular-shaped pouch that lies between the vestibular fold and the inner plate of the thyroid cartilage.3 The saccules contain mucous glands that help lubricate the vocal folds.5
Vocal folds
The vocal folds extend from a midline point on the inner surface of the thyroid cartilage, or the anterior commissure, to the vocal process of the arytenoid cartilage. The anterior commissure corresponds approximately to the midway point between the thyroid notch and the lower border of the thyroid cartilage at the midline. The conus elasticus is the lateral portion of the cricothyroid ligament. It extends from the anterior arch of the cricoid cartilage to the thyroid cartilage anteriorly and to the vocal process of the arytenoid posteriorly. The thickened superior free margin of the conus elasticus is also known as the vocal ligament. Running parallel and inferolateral to the vocal ligament is the vocalis component of the thyroarytenoid muscle. The glottis is the space between the vocal folds. The anterior three-fifths of the glottis is termed the membranous vocal cord, or the vocal fold, whereas the posterior two-fifths is termed the cartilaginous vocal cord, or the respiratory glottis (Figure 1.2).6 The vocal folds are usually bulkier and longer in adult males, resulting in a deeper voice. Note: Currently the terms vocal ‘fold’ and vocal ‘cord’ are used synonymously by laryngologists and as yet there is no consensus on terminology.
Skeleton of the larynx
Thyroid cartilage
The thyroid cartilage is formed by two quadrangular laminae that join anteriorly to form the laryngeal prominence (Adam’s apple). The angle between the lamina is more acute in adult males, hence a more prominent Adam’s apple. They separate superiorly to form the thyroid notch. Posteriorly, the laminae project both upwards and downwards to form the superior and inferior horns. A small facet is located on the medial surface of the inferior horn that articulates with the cricoid cartilage.

Figure 1.1 Laryngeal subdivisions. Coronal section of the adult larynx (viewed from posteriorly) showing the supraglottis, glottis and subglottis regions.

Figure 1.2 Vocal cords. Schematic endoscopic view of the larynx showing subdivisions of the vocal cord.
Cricoid cartilage
The cricoid cartilage is the only complete cartilaginous ring in the human airway. The cartilage is composed of the narrow cricoid arch anteriorly, which measures 5–7 mm in height7, and a wider quadrate lamina posteriorly, which measures approximately 21 mm in females and 25 mm in males.8 At the junction between the lamina and the arch is a small round facet that articulates with the lower horn of the thyroid cartilage. The superior margin of the lamina contains two smooth concave facets that articulate with the base of the arytenoid cartilage. These are synovial joints and therefore are susceptible to arthritis and ankylosis.
Arytenoid cartilages
The arytenoid cartilages are pyramidal in shape and have three surfaces, an apex and a base. They lie on the posterior aspect of the larynx on the superior margin of the lamina of the cricoid cartilage. The anterior and lateral angles of the base elongate to form the vocal and muscular processes, respectively. The vocal ligaments attach to the vocal process, whereas the posterior and lateral cricoarytenoid muscles attach to the muscular process.
Epiglottis
The epiglottis is a thin, leaf-shaped fibrocartilage that lies in the upper part of the larynx and behind both the hyoid bone and the base of the tongue. Its pointed inferior stalk is called the petiole, and is attached to the inner surface of the thyroid cartilage via the thyroepiglottic ligament. It is anchored to the posterior surface of the hyoid bone via the hyoepiglottic ligament. Its free superior portion is covered by mucosa, which forms the anterior border of the laryngeal inlet.
The minor cartilages of the larynx
The corniculate cartilages are two small cartilages that articulate with the apex of the arytenoid cartilage. The club-shaped cuneiform cartilages are located within the aryepiglottic fold.
Hyoid bone
The hyoid bone is a horseshoe-shaped bone suspended in the anterior most part of the neck by the suprahyoid and tongue muscles. It contains a quadrilateral curved central body and the lateral greater and lesser horns. The hyoid bone’s anterior surface is convex with a median ridge, whereas the posterior surface is smooth and concave. Numerous muscles, membranes and ligaments attach to the hyoid bone.
Muscles of the larynx
The muscles of the larynx can be classified as extrinsic or intrinsic muscles. The extrinsic laryngeal muscles have attachments outside the larynx. They include the strap muscles of the neck, the stylopharyngeus, the palatopharyngeus and the inferior constrictor muscles. The extrinsic muscles move the larynx as a whole and play a role in breathing and swallowing.
The origin and insertion for intrinsic muscles are confined to the larynx. Although their main functions are adduction, abduction and adjusting vocal fold tension (Figure 1.3), they can help modulate the laryngeal inlet as part of the airway protection mechanism.

Figure 1.3 Actions of the laryngeal muscles. Posterior view of the relationship of the laryngeal muscles to the arytenoid cartilage. TA, thyroarytenoid; LCA, lateral cricoarytenoid; PCA, posterior cricoarytenoid; IA, interarytenoid.
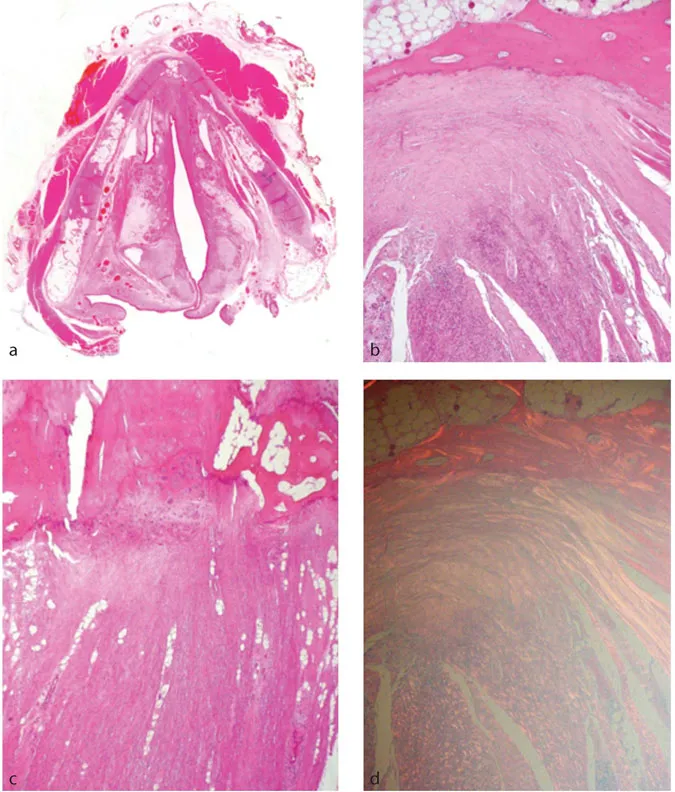
Figure 1.4a–d Broyle’s ligament. The anterior commissure tendon fibres can be seen inserting into cartilage. The arrangement of the collagen fibres is well demonstrated when viewed under polarised light (d).
Thyroarytenoid muscles
The thyroarytenoid muscles originate from the anterior commissure tendon (or Broyle’s ligament) on the internal surface of the thyroid cartilage (Figures 1.4a–d) and run posteriorly to insert on the arytenoid cartilage. The majority of the muscles’ fibres run lateral to the vocal ligament and constitute the vocalis muscle. The upper division of the muscle, which varies among individuals, runs in the aryepiglottic fold, vestibular folds and lateral to the laryngeal ventricle.
The primary function of the thyroarytenoid muscle is to shorten the vocal ligament and adjust vocal fold tension during phonation. Furthermore, muscle contraction can rotate the arytenoid cartilage inwards to close the glottis.
Posterior cricoarytenoid muscles
The posterior cricoarytenoid muscles extend upwards and laterally from the posterior surface of the cricoid lamina and insert on the muscular process of the arytenoid cartilage. The posterior cricoarytenoid muscles are the only vocal fold abductors. The more horizontal superior part of these muscles rotate the arytenoid cartilage laterally, thereby abducting the vocal folds, whereas the vertical inferior fibres pull the arytenoids over the upper margin of the cricoid, which moves them apart.
Lateral cricoarytenoid muscles
The lateral cricoarytenoid muscles originate from the upper border of the arch of the cricoid cartilage and insert on the muscular process of the arytenoid. They rotate the arytenoid medially to close the glottis.
Interarytenoid muscle
The interarytenoid muscle is the only unpaired intrinsic muscle. It runs posteriorly between the muscular processes of the arytenoids. Its main function is to adduct the vocal folds by approximating them.
Cricothyroid muscles
The cricothyroid muscles originate from the anterolateral surface of the cricoid cartilage arch. The fibres pass superior and dorsal to insert on the oblique ridge of the thyroid cartilage. While all the other intrinsic larynx muscles are innervated by the recurrent laryngeal nerve, the cricothyroid is innervated by the external branch of the superior laryngeal nerve.
Joints of the larynx
Cricothyroid joint
The inferior horn of the thyroid cartilage articulates with the cricoid cartilage at an encapsulated synovial joint. The cricothyroid joint allows both rotation and glide movement. Contraction of the cricothyroid muscles leads to forward and downward tilting of the thyroid cartilage and a simultaneous upward movement of the cricoid.
Cricoarytenoid joint
The cricoarytenoid joint (CAJ) is a synovial articulation between the base of the arytenoid cartilage and the lamina of the cricoid cartilage. The joint has a loose capsule inserting at a distance from the cartilage articulation surface margin, allowing a wider range of movement.9 The arytenoid cartilage can glide forwards and backwards over the cricoid lamina, rock medial and lateral and rotate around its axis. The capsule of the CAJ is reinforced by the posterior cricoarytenoid ligament. Desp...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Table of Contents
- Contributors
- Foreword
- Preface
- About the editors
- Abbreviations
- Chapter 1: Basic science
- Chapter 2: Voice assessment in the out-patient department
- Chapter 3: The professional voice user
- Chapter 4: Benign vocal fold lesions
- Chapter 5: Neurological and neuromuscular disorders of the larynx
- Chapter 6: Vocal fold paralysis
- Chapter 7: Principles of speech and language therapy
- Chapter 8: Swallowing disorders
- Chapter 9: Laryngeal trauma
- Chapter 10: Laryngotracheal stenosis
- Chapter 11: Extra-oesophageal reflux
- Chapter 12: Infections of the larynx
- Chapter 13: Recurrent respiratory papillomatosis
- Chapter 14: Inflammatory disorders of the larynx
- Chapter 15: Dysplastic lesions of the larynx
- Chapter 16: Paediatric laryngeal disorders
- Chapter 17: In-clinic procedures
- Chapter 18: Anaesthetic considerations in laryngology
- Chapter 19: Gender dysphoria and the larynx
- Chapter 20: New horizons in laryngology
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Practical Laryngology by Declan Costello, Guri Sandhu, Declan Costello,Guri Sandhu in PDF and/or ePUB format, as well as other popular books in Medicine & Audiology & Speech Pathology. We have over 1.5 million books available in our catalogue for you to explore.