Genital prolapse, or pelvic organ prolapse, occurs when the structures of the pelvis protrude into the outside vaginal canal. Genital Prolapse and Urinary Incontinence is the first book of its kind dedicated specifically to genital prolapse and is filled with every different type of prolapse, including the bladder, uterus, rectum, and
eBook - ePub
Female Genital Prolapse and Urinary Incontinence
- 272 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Female Genital Prolapse and Urinary Incontinence
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Part 1: Introduction
1
Dynamic Anatomy of the Pelvic Floor
Michel Degueldre and Jean Vandromme
Obstetrics and Gynecology Department, University Hospital St. Pierre, Brussels, Belgium
Bruno J. van Herendael
ZNA Stuivenberg, Antwerp, Belgium and Gynecology Department, Università dell’Insubria, Varese, Italy
INTRODUCTION
Before taking off it would be interesting to know how to land.
—Arnaud Wattiez
Multiple challenges await the surgeon who operates on the pelvic area. Although specific anatomical landmarks define the limits of the operating field as in any other surgical field, very specific situations exist in this area:
▪ Nerve-sparing surgery becomes mandatory to retain the function of the different organs.
▪ Pressure gradients in the different compartments play an important role in the postoperative success rate for suspension surgery.
▪ The anatomical and functional interaction of the organs is very important to guarantee normal function of both the sexual and voiding aspects of daily life.
These factors make pelvic surgery in the female a challenge. A thorough knowledge is necessary not only of pelvic anatomy, vascular-nervous-muscular-ligamental-fascial-virtual and physical spaces (foramina), and bony structures, but also of the mechanical forces and physiological processes.
Pelvic surgeons have to realize that there exist two different anatomies: the one that is described in anatomy books and observed in cadaver dissections and the one that is encountered during surgery. We need to find specific solutions for the specific patient.
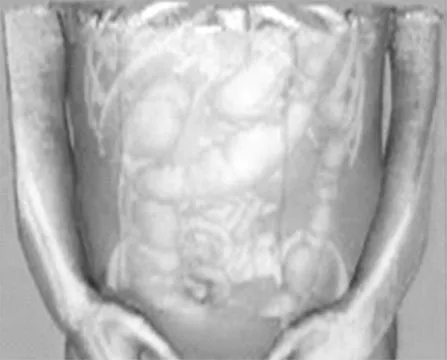
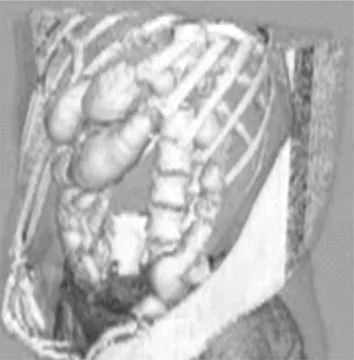
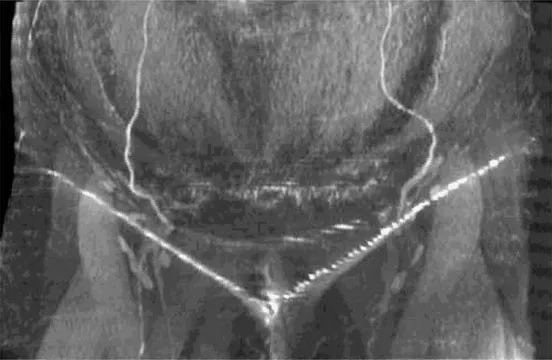
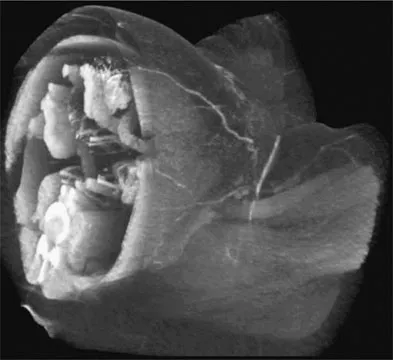
It would be ideal to have a three-dimensional virtual reality picture of the patient’s anatomy to properly assess the condition before making surgical decisions (Figs. 1,2,3).
Virtual reality imaging is not yet available, but the spiral CT scan provides detailed imaging (Figs. 4,5,6,7). Computer software programs provide the capability to produce moving images from the sequence of still pictures. By sailing through the tissues the viewer gets the impression of a virtual reality image.
The aim of this chapter is to provide a pictorial description of the female pelvis combining anatomical, physiological, and functional data.
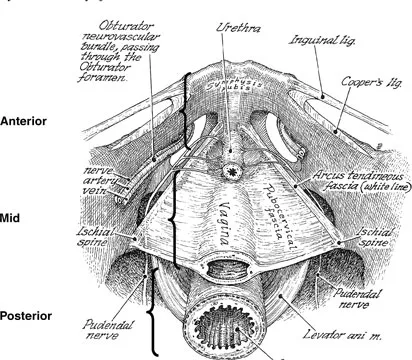
The pelvis of the human female is divided into three functional entities: (i) the anterior compartment; (ii) the mid compartment; and (iii) the posterior compartment (Fig. 8).
The Anterior Compartment
Bone: Starting front to back this compartment contains: the pubic bone, consisting of the superior pubic ramus, the pectineal line (pectin Ossis pubis) ending median in the pubic tubercle, the crista obturatoria, the inferior pubic ramus and the ramus of the ischial bone.
Foramina: The main foramen in the anterior compartment is the obturator foramen delineated anteriorly by the superior pubic ramus and the inferior pubic ramus. This entity is sealed by the obturator membrane and leaves openings superior and lateral under the superior ramus: the obturator channels.

Fascia: These include the urogenital fascia (inferior and superior fascia diaphragmatis urogenitalis), which incorporate the median and lateral pubovesical ligaments anteriorly; the vesicocervical fascial fibers (pubocervical or urogenital); and the tendineus arch of the levator ani muscle. The fascia is the border between the anterior and mid compartments.

Ligaments: The symphysis pubis with the superior pubic ligament and Cooper’s ligaments over the superior pubic ramus are the more important landmarks for the surgeon. The other ligaments encountered when moving from anterior to posterior are: the median and lateral pubovesical ligaments, the inguinal ligament (Poupart’s), and the round ligament over its most distal part in the inguinal canal. There are also the arcuate pubic ligament and the transverse perineal ligament.
Muscles: Laterally from the exterior toward the center are the obturator muscle and the anterior aspect of the levator ani muscle. Anteriorly and superiorly are the layers of the rectus abdominal muscle. The deepest part of the female pelvis is closed, anterior by part of a transverse muscle layer surrounding the genital hiatus composed of the ischio-cavernosus, laterally and the bulbo-spongiosus delineating the vagina. Both muscles rest on and are part of the deep transverse perineal muscle.

Nerves: Knowledge of the location and function of the various neural structures and their preservation are essential for the successful outcome of the surgical intervention. The neurological structures of this compartment are: the femoral nerve, the ilio-inguinal nerve, superficial and deep branches of the perineal nerve, the perineal branch of the posterior femoral cutaneous nerve, and the pudendal nerve (somatic) from the sacral plexus (S2–S4). Both sensory and somatic fibers from the lower vagina and the perineum accompany the pudendal nerve. The urinary bladder and the lower ureter are serviced by pre- and post-ganglionic sympathetic and parasympathetic fibers.
▪ Parasympathetic from S2-S3-S4 (vesical plexus) responsible for transudation at the vaginal level and erection at the level of the clitoris.
▪ Sympathetic from L1 to L2: the plexus hypogastricus superior ending in the nervus hypogastricus to form the plexus hypogastricus inferior and the plexus uterovaginalis (plexus of Frankenhäuser) terminating in the nervus vaginalis. The main action of these sympathetic fibers is contraction.
▪ Somatomotoric and somatosensitive: from S2 to S4 the nervus pudendus ending at this level in the nervus dorsalis clitoridis and the nervi labiales posteriores. The main action of the nerve fibers is contraction.
Vessels: Superior and inferior vesical arteries and veins (branches respectively of the umbilical artery and vein and the middle rectal artery and vein) supply the bladder. The vagina gets its blood supply through the vaginal artery and vein (branches of the internal iliac artery and vein). The anterior compartment also contains the inferior epigastric artery and vein (branches of the external iliac artery and vein), a structure best avoided during laparoscopic entry.
Lymphatic structures: The most important lymphatic structures of this compartment are the inguinal nodes; the most distal of...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Foreword
- Preface
- Table of Contents
- Contributors
- PART I: INTRODUCTION
- PART 2: THE ANTERIOR SEGMENT
- PART 3: THE MID SEGMENT
- PART 4: THE POSTERIOR SEGMENT
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Female Genital Prolapse and Urinary Incontinence by Victor G. Gomel, Bruno van Herendael, Victor G. Gomel,Bruno van Herendael in PDF and/or ePUB format, as well as other popular books in Medicine & Gynecology, Obstetrics & Midwifery. We have over 1.5 million books available in our catalogue for you to explore.