Given the prevalence of substance abuse in general clinical populations, it is important for healthcare providers to have knowledge and skill in the treatment of these problems. Evidence-Based Practice (EBP) involves the integration of the best evidence with clinical expertise and patient values. This text is designed as a bridge for practitioners that will provide up-to-date evidence reviews as well as information on how to best keep up with emerging trends in the field. The editors have gathered expert authors to provide a much needed summary of the current status of the evidence based practice for both the assessment and treatment of specific substance use disorders.
eBook - ePub
Pharmacology and Treatment of Substance Abuse
Evidence and Outcome Based Perspectives
- 702 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Pharmacology and Treatment of Substance Abuse
Evidence and Outcome Based Perspectives
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Part I
Psychopharmacology and Neurobiology of Substance Abuse
Alice M. Young
Texas Tech University and Texas Tech University Health Sciences Center
Texas Tech University and Texas Tech University Health Sciences Center
The chapters in this introductory section focus on conceptual models in pharmacology and psychopharmacology, and on how interactions among key behavioral, cellular, genetic, neuronal, and physiological processes contribute to substance use problems. The section begins with overviews of basic principles of drug action and of drug effects linked to substance abuse and dependence, and it finishes with discussions of the neurobiology and genetics of addiction. The breadth of these discussions illustrates that all drugs have multiple effects that can affect functions of multiple body systems and that are modified by the individual user’s own particular biology, psychology, and experience.
All of the research knowledge described in this section relies on a framework of ethical, legal, research, and theoretical practices that protect vulnerable research participants. These chapters draw from in vitro studies of drug effects in cell cultures and brain tissues, from laboratory studies of behavioral and psychological effects of drugs in humans and other animals, and from clinical studies both in individuals who meet diagnostic criteria for substance use disorders and also in healthy research participants who have no history of substance abuse or misuse. By U.S. and international law, research with humans or animals is subject to rigorous review by Institutional Review Boards (for human participants) or Institutional Animal Care and Use Committees (for vertebrate animal subjects). Research involving administration of abused drugs is also subject to federal, state, and local controlled substance regulations. Ongoing development of our framework of ethical, legal, research, and theoretical practices will be critical to advancing research in this area and to translating research into clinical assessment and treatment.
Chapter 1 introduces key concepts of pharmacokinetics and pharmacodynamics. Paronis provides broad coverage of the principles of drug action, which in turn provide the foundations for the research strategies described in later chapters. Readers will quickly appreciate that drug effects are emergent effects, resulting from interactions of drugs and our normal biological processes, and that understanding the principles of drug actions will enable critical appreciation of theoretical and research approaches to treatment.
In Chapter 2, Cooper and Comer highlight the contributions that behavioral theory and research have made to development of potential pharmacotherapies for substance use disorders. They point out that the direct aim of a pharmacotherapy is to support and maintain abstinence from drug use, and argue that identification of such pharmacotherapies benefits from human laboratory studies that draw on the rich tradition of theory-based studies in animals. The chapter reviews the range of human laboratory models that do, or do not, provide predictive evidence of treatment effectiveness.
In Chapter 3, Vandrey and Mintzer address the clinical concern raised by impairments in cognitive functioning produced by abused drugs and drug abuse. They review what is known about which cognitive processes are affected by which drugs and under what conditions, about the impact of altered functioning on daily or specialized functioning, and about the relative severity of these effects across drug classes. In a discussion especially relevant to this volume, they discuss emerging evidence about whether drug effects on cognitive functioning may affect cognitive skills required by cognitive-behavioral or psychosocial treatment modalities.
Drug abuse and misuse can be accompanied by tolerance, sensitization, and/or physiological dependence. In Chapter 4, Allen draws upon research with animals and humans to guide the reader to a balanced understanding of these adaptive processes. As noted by Allen, brains and behaviors adapt in many ways to drug exposure, and an individual’s specific learning opportunities play major roles in whether, when, and how tolerance and/or sensitization to effects of drugs occur. Moreover, the contributions of these processes to addiction are under vigorous scientific debate.
In Chapter 5, Koob provides a detailed conceptual model of how changes in biological and neurobiological processes mediate an individual’s transition from occasional drug use to addiction. This evolving model begins with detailed information about how drug use engages normal brain circuits, learning processes, and neurochemical processes. The model then incorporates the critical feature that repeated use of addictive drugs changes how these processes operate, thereby creating a new trajectory that recruits new systems and motivational states. The proposed stages of addiction and accompanying brain changes provide a theory-driven model to guide both basic and clinical research.
In Chapter 6, Ray and Hutchinson address another rapidly changing area, the genetics of addiction. They begin with an overview of basic principles of genetics and then review the complex work that will be required to unravel how a genetic variant acts to influence the risk and course of addiction in an individual. A major theme of this chapter is the likelihood that interactions among environments, genes, and behaviors are not unidirectional. A second theme is that genetic variation may either accelerate or slow changes in the neurobiological/ psychological processes that shape or treat addiction.
Together, these chapters provide a conceptual review and background of biological and psychological processes that interact in addiction and substance abuse. Identification of potential substance use treatments builds upon the models and conceptualizations covered here. The evidence associated with substance use treatment is the focus of the remainder of this volume.
1
Principles of Drug Action: Pharmacokinetics and Pharmacodynamics
Carol A. Paronis
Northeastern University
Northeastern University

Pharmacokinetics
Pharmacokinetic aspects of drug action concern the bioavailability of drugs, including how drugs are absorbed into, distributed throughout, and eventually metabolized and eliminated from the body. These processes are sometimes referred to in the aggregate by the acronym absorption, distribution, metabolism, excretion (ADME) and they establish the potency of drugs and the time course of the effects of drugs. Pharmacokinetic characteristics of drug action are determined in part by the physicochemical properties of the drug and in part by the physiology of the organism, which may be altered either intentionally or inadvertently. For example, a drug that has a fast onset and short duration of action may have its time course of activity altered by being chemically reformulated as a slow-release tablet. Alternatively, a drug that is expected to have effects that last eight hours based on studies in healthy individuals might last three days in someone suffering from liver failure. Despite these potential variations in pharmacokinetic properties, the principles introduced below generally apply in describing how drugs reach their site of action by being absorbed into, and distributed by, the circulatory system, and how drug action is terminated by metabolism to inactive products which are then eliminated from the body.
Administration
The administration of drugs refers to the process by which drugs are delivered to an organism. There are several different methods that can be used to deliver drugs, and the best route of administration varies according to the intended purpose for which the drugs are being administered. In humans, the most common routes of administration are oral (per os; PO), injection into the bloodstream (intravenous; IV), injection under the skin (subcutaneous; SC), injection into muscle (intramuscular; IM), or mucosal absorption, which occurs when a drug is taken by inhaled or buccal routes. A less common route of administration, but one that has application to substance abuse, is transdermal administration, in which a drug is slowly released from a patch and absorbed into the bloodstream through the skin. Each method of administering drugs has unique advantages and disadvantages, and all will differentially influence the rate at which drugs are absorbed into the bloodstream and the percentage of drug taken that ultimately enters the circulation, referred to as the bioavailability of the drug (see Figure 1.1).
Injection of drug by any of the routes mentioned above, IV, SC, or IM, is generally followed by a rapid and constant rate of absorption into the bloodstream. Of the common injection routes, IV administration results in the fastest onset to drug action with zero time to absorption as the drug is delivered directly to the bloodstream. IV administration also presents the best way to deliver precise doses of drugs; a drug administered by IV route is considered to be completely absorbed and therefore has 100% bioavailability (Levine, 1983). Injection of drugs by SC or IM routes also tends to result in relatively fast onset to action, although this can depend on the vehicle by which they are administered. “Vehicle,” here, means the substances in which a drug is dissolved or otherwise formulated, serving the function of increasing the volume of the dose to be delivered. In most cases, drug vehicles are inert and do not influence direct effects of the drug; however, they can have physical properties that affect the drug absorption into the blood. Most drugs are dissolved in an aqueous solution and are rapidly absorbed, on the order of minutes. On occasion, however, drugs injected IM or SC may be formulated as suspensions which provide a slower absorption into the circulatory system. This slow absorption can allow drug effects that are sustained for days or even months. In addition to this ability to manipulate absorption by varying the vehicle, another advantage of administering drugs by injectable routes is the avoidance of “first-pass metabolism” in the liver. Disadvantages associated with drug injection include relatively high costs and the inherent risks of infection or other irritation occurring at the site of injection.
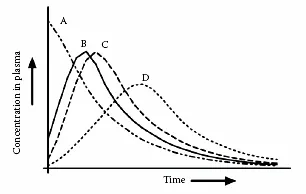
Figure 1.1
Theoretical plasma concentration of a drug following different routes of administration; IV (curve A), SC (curve B), IM (curve C), and PO (curve D). Drug administered IV is immediately and fully absorbed, yielding a large peak concentration that is cleared from the plasma relatively quickly. Oral administration produces the lowest peak concentration, but retains measurable concentrations for the longest period of time.
Theoretical plasma concentration of a drug following different routes of administration; IV (curve A), SC (curve B), IM (curve C), and PO (curve D). Drug administered IV is immediately and fully absorbed, yielding a large peak concentration that is cleared from the plasma relatively quickly. Oral administration produces the lowest peak concentration, but retains measurable concentrations for the longest period of time.
Oral administration is the most common method of taking drugs, either as therapeutics or as abused substances. Oral administration presents an easy and economical way to deliver drugs and virtually every drug can be taken orally. Despite its ease of use, however, oral drug administration has several disadvantages, including variable rates of absorption and low drug bioavailability. Drugs that are taken orally are sometimes absorbed into the bloodstream over minutes or sometimes hours, depending on the rate of gastric emptying, which, in turn, depends on a number of factors including the amount and type of food in the stomach, the gastric pH level, and the position and activity of the body. The rate of absorption can further vary as a function of the physicochemical properties of the drugs, especially their degree of ionization. Most drugs exist as weak acids or weak bases at a pH of 7.4, the normal pH of plasma, but in some organs, including the stomach and kidneys, the pH varies. In the stomach, the pH level decreases when food is eaten, changing the ionization of drugs, such that acids become less ionized and bases become more ionized at the lower pH. Hence, acids are more likely to diffuse into the blood and bases are less likely to enter the bloodstream after food is eaten (Levine, 1983). In addition to this variable absorption, bioavailability of drugs is almost always very low following oral administration because substances that enter the bloodstream from the alimentary canal must pass through the liver before being distributed to other tissues and organs in the body. Although drugs are metabolized throughout the body, the liver is the organ primarily associated with drug metabolism. Because orally delivered drugs enter the liver before the general circulation, it is often the case that a high percentage of the orally administered drug is metabolized to inactive products within the liver and eliminated from the body without ever producing a biological effect. This process, by which the drug is lost before entering the general circulation, is termed “first-pass metabolism.”
Transmucosal administration is not a very common method for delivering therapeutics; however, it is the manner by which some drugs that are inhaled are absorbed into the circulation. Drugs that are available as vapors or aerosols, such as smoked nicotine, or as powders that are taken intranasally, are absorbed directly into the bloodstream from the mucosal membranes lining the mouth or nasal passages. Some drugs, for example nicotine gum, are administered buccally, that is they are taken by mouth but not swallowed, and these also are absorbed through mucosal linings. Because this route of administration avoids first-pass metabolism by entering the bloodstream at or near the site of administration, a drug that is administered by inhalation or buccally can be expected to have pharmacokinetic characteristics—high bioavailability and rapid onset to action—similar to those seen following injectable routes of administration.
In contrast to the rapid absorption seen with transmucosal administration, the slowest absorption of drugs occurs when a drug is administered using transdermal patches. Drug patches are comprised of multiple layers, including an impermeable outer layer, a drug reservoir, a porous membrane that controls the rate of release of the drug, and an adhesive to secure the patch to the skin. When the patch is affixed to the skin, the drug diffuses out of the reservoir, through the porous membrane, to the surface of the skin. The skin is nearly impermeable to all substances and so the movement of the drug particles across the skin and into the underlying blood vessels is very slow. One advantage of this method of drug delivery is that the steady release of the drug is excellent for maintaining consistent levels of the drug in blood for a period of weeks. However, in addition to the slow onset, other disadvantages of this route of administration are that patches must be formulated with very large quantities of drug and the dose cannot be easily adjusted for individuals. The transdermal route of administration has somewhat limited clinical utility, although it is an excellent way of delivering drugs for indications requiring constant blood levels of drugs for long periods of times, or when patient compliance is a concern. Patches originally were used to deliver scopolamine prophylactically for motion sickness; more recent indications for patch drug delivery systems are nicotine for smoking reduction, fentanyl for pain alleviation, and hormonal combinations for birth control (Gilman, Rall, Nies, & Taylor, 1993; Shiffman, Fant, Buchhalter, Gitchell, & Henningfield, 2005).
Absorption and Distribution
After a drug is administered, it is distributed throughout the body within the plasma, the liquid component of blood. Drugs enter or leave the plasma by diffusing across the biological membranes. The diffusion can be passive, by flowing from an area of high concentration to an area of low concentration without restriction, or it can be facilitated by coupling to other molecules in the body, called carrier proteins, that help transport substances across membranes that otherwise act as barriers to the substances due to their size, solubility, or ionization. The probability that a drug will diffuse across a membrane is determined not only by the concentrations of the drug on either side of the membrane, and of other molecules found in the blood or organ tissues, but also by the chemical structure of the drug, the composition of the membranes, and other physiological factors.
Most biological substances enter or leave the bloodstream within the capillaries, the smallest vessels of the circulatory system. The function of the capillaries is to allow the exchange of nutrients or other products between the circulating blood and the cells of other organs and so most solutes pass through the capillary walls easily. Both organic and inorganic substances, including drugs, can diffuse across the capillary membrane by going either through or between the capillary cells, depending on whether the substances are hydrophilic (water-loving) or hydrophobic (water-fearing). Like most cells in the body, the membranes of the capillary cells are comprised primarily of phospholipids, which are lipid molecules with charged head groups, oriented such that the lipids are internalized within the membrane and the charged head groups are found along the intracellular and extracellular surfaces of the cell. This arrangement results in a polar, or hydrophilic surf...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Series Editor Preface
- Foreword: The Transdisciplinary Perspective
- Part I: Psychopharmacology and Neurobiology of Substance Abuse
- Part II: Conceptual Models and Principles of Substance Abuse Treatment
- Part III: Assessment and Treatment of Substance Abuse
- Part IV: Special Topics
- About the Editors
- About the Contributors
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Pharmacology and Treatment of Substance Abuse by Lee M. Cohen, Frank L. Collins, Jr., Alice Young, Dennis E. McChargue, Thad R. Leffingwell, Katrina L. Cook, Lee M. Cohen,Frank L. Collins, Jr.,Alice Young,Dennis E. McChargue,Thad R. Leffingwell,Katrina L. Cook in PDF and/or ePUB format, as well as other popular books in Psychology & Pharmacology. We have over 1.5 million books available in our catalogue for you to explore.