This chapter provides an introduction to the aspects of Asperger syndrome that will most concern readers of this book. The main focus is on the problems and challenges faced by people with this condition, and helping them to understand the adjustments they need to make when they move from school to college or university.
What is Asperger syndrome?
Asperger syndrome is an autism spectrum disorder. It was first described by an Austrian psychiatrist, Hans Asperger, in 1944 in his paper, ‘Autistic Psychopathy in Childhood’, but it was some 40 years before information about the condition began to be widely disseminated in the fields of education and psychology.
Asperger described four boys who had a ‘fundamental disturbance in common’ resulting in severe difficulties with social integration. Often the boys’ social problems were so profound that they dominated their lives. Asperger stated that in some cases a ‘high level of original thought and experience’ compensated for social problems. He also stressed that people with these social difficulties can ‘fulfil their social role within the community especially if they find understanding, love and guidance’. Although Asperger did not relate autistic psychopathy to intelligence in 1944, in a later paper (1979) he recorded his observation that children with ‘infantile autism’ had a propensity to high intelligence with special abilities in areas of logic and abstraction.
Dr Lorna Wing (1981) was the first person to use the term ‘Asperger’s syndrome’ to describe 34 individuals whose profile resembled that of the four boys described by Asperger in 1944. She concluded that an individual could be autistic and yet still have considerable abilities in language, cognitive skills and social interest. Since Uta Frith’s English translation of Asperger’s original study was published (Frith 1991) the condition has become increasingly recognised in the English-speaking world. Recent scientific and media attention has now brought Asperger syndrome into the wider public domain.
Asperger syndrome is characterised by the presence of three major functional impairments, in the absence of general learning difficulties. These impairments occur in:
- • social interaction and social relationships
- • verbal and non-verbal communication
- • imagination, behaviour and flexibility of thought.
There continues to be some confusion about the terminology used to describe individuals with autistic features who have superficially good language skills and average or above-average cognitive abilities. Throughout this book the term ‘Asperger syndrome’ will be used, rather than terms which are often used synonymously, such as high-functioning autism, autistic continuum disorder, autism spectrum disorder, atypical autism and mild autism. Using the label ‘mild’ to describe an autistic disorder significantly understates the severity of the problems encountered by people with Asperger syndrome and their families, who do not consider their disorder to be mild in any way.
Hans Asperger stressed the developmental characteristics of the syndrome he described; as individuals grow older and mature, their profile of strengths and difficulties changes. Strategies and support systems that were appropriate at a particular stage of development, for example at primary school, will need to be monitored, evaluated and adjusted on an on-going basis as the child passes from adolescence to adulthood.
‘I like the way I think for the most part, and the fact that I have Asperger syndrome doesn’t bother me – I am happy that I can see many things that so-called “normal people” can’t see. I won’t be able to forget about having Asperger’s – ever. It’s me and that’s it.’ EM
Asperger strongly believed that the children he studied had the potential to grow up to be successful in their working lives and to make a positive contribution to society. He was convinced that their future success was dependent on appropriate education and support based on a thorough knowledge of their strengths and weaknesses.
Diagnosis of Asperger syndrome
A key aspect of the diagnosis of Asperger syndrome is that, while there are diagnostic criteria, there is no single formal diagnostic process. Members of different professions have developed an interest in Asperger syndrome, including paediatricians, psychologists, psychiatrists, speech and language therapists and specialist teachers. Many of these people may consider that they have sufficient expertise to make a diagnosis. There are as yet no regulations as to the professional qualifications required to make a diagnosis. This means that informed individuals may suspect the syndrome and make an informal diagnosis without seeking professional advice or confirmation.
A diagnosis of Asperger syndrome is rarely made before a child is five years old, and the syndrome is more frequently identified after a child has been at school for a few years. Children who are eventually diagnosed may previously have been thought of as different in some way, for example autistic, hyperactive or presenting with unusual behaviours.
There has been a significant increase in the diagnosis of Asperger syndrome in recent years. The incidence of the syndrome is unlikely to have changed but greater public and professional awareness, including clearer diagnostic criteria and tools, has had this effect. The current consensus is that Asperger syndrome affects approximately 1 in 250 of the population, with a ratio of six males to one female (Gillberg 2002).
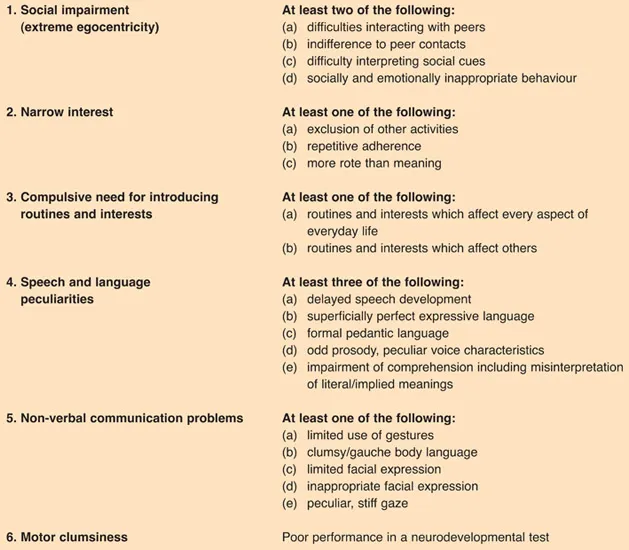
Hans Asperger did not suggest formal diagnostic criteria. Lorna Wing (1988) described the syndrome and its various manifestations in detail but she did not lay down specific criteria for diagnosis either. It was only 15 years ago that Gillberg and Gillberg (1989) set out specific diagnostic criteria, focusing on six categories of impairment. According to Gillberg (1991), five out of the six impairments need to be present to make a definitive diagnosis. (See Box 1.)
These six categories are sub-divided into twenty specific symptoms listed in Box 1, of which at least at least nine have to be present for a positive diagnosis.
Diagnostic criteria for Asperger syndrome first appeared in the International Classification of Diseases and Disorders (ICD-10) published by the World Health Organisation in 1993 (WHO 1993). The following year the disorder was included in the Diagnostic and Statistical Manual (DSM-IV) (American Psychiatric Association 1994).
Both the ICD-10 and the DSM-IV specified that a diagnosis of Asperger syndrome could only be made if the criteria for autism were not met. The ICD-10 also emphasised the significance of a history of normal language and social development in the first three years of life. However, in a clinical setting it is unusual for children presenting with Asperger syndrome to have had unremarkable cognitive, linguistic and social development in these early years. They are likely to have developed language skills which may appear extremely advanced, but the type of language and their social use of this language are frequently unusual. For example, the ability to recite large sections of dialogue from a favourite video such as Thomas the Tank Engine, with perfectly replicated words, accents and intonation patterns, does not necessarily indicate an ability to engage in functional conversation. Speech is often described as being pedantic and quaint, with little awareness of a conversational partner.
Some people for whom a diagnosis of Asperger syndrome would be appropriate may not meet all the diagnostic criteria, as individual personality traits and cognitive strengths and weaknesses may distort the clinical picture. There is also thought to be some variation in the clinical profile according to gender. Gillberg reports that in his experience
… girls with Asperger syndrome are sometimes less aggressive, less prone to hyper-activity and are not so fixated on specific narrow interests. They tend to be more interested in ‘social’ toys, such as dolls, whereas boys often demonstrate a stronger interest for hard objects, water, sand and mechanical things. (Gillberg 2002)
It may also be particularly difficult to differentiate Asperger syndrome from some other developmental disorders, such as autism and attention deficit hyperactivity disorder (ADHD). It is possible that hyperactivity and impulsiveness camouflage some of the social difficulties encountered in Asperger syndrome; however, when the hyperactivity is treated with medication, the social problems become more apparent.
Genetic studies have revealed that many people diagnosed with an autism spectrum disorder have close relatives who exhibit some manifestations of Asperger syndrome without meeting the full diagnostic criteria. Personality traits such as eccentricity, social withdrawal, preoccupying interests and obsessions are often identified in the extended family. This is often referred to as the broader phenotype (or lesser variant) of autism.
‘It was a huge relief when I was finally diagnosed with Asperger syndrome. I had known all my life that I was different and couldn’t relate to other people but I didn’t understand why I was so different.’ EM
With increasing media exposure and the availability of books and articles about Asperger syndrome readily available, many adults are now being diagnosed for the first time. As mo...