![]()
CHAPTER 1
Autism
An introduction
Purpose of the book
This book sets out to provide parents and professionals with an insight into the nature and educational implications of autism, particularly as it presents in very young children. Consideration will be given to the issues surrounding assessment and diagnosis.
In addition, the book aims to equip early years practitioners and parents with knowledge of a range of intervention strategies to promote learning, social development, communication and appropriate behaviour. The book goes on to explore the possibilities for enhancing access to the early years curriculum.
History
There is no doubt that there have been people with autism throughout history. However, it was not until the 1930s that the first systematic study of autism took place in Boston, USA. Leo Kanner reported the findings of this study in 1943 in his paper ‘Autistic Disturbance of Affective Contact’.
Kanner was a pioneer in the field of child psychiatry. His study began in 1938 when a fascinating five-year-old, Donald, was brought to his clinic. From the age of two-and-a-half, Donald had been able to list the names of all the US Presidents, say the alphabet backwards and forwards, and recite the twenty-third Psalm – although he was unable to carry on a normal conversation. Over the next few years, Kanner saw ten more children who displayed similar behaviour patterns. Their parents commented they were ‘self-sufficient’, ‘like a shell’, ‘happiest when left alone’, ‘acting as if people weren't there’, ‘giving the impression of silent wisdom’.
Kanner's paper was circulated, discussed and reviewed within the psychiatric world and considered an important breakthrough in the understanding of children who up to this time had appeared beyond help. Kanner used the term ‘early childhood autism’ which he may have felt emphasised both the time of the first manifestations of the disorder and the child's limited accessibility.
For Kanner the defining features of autism were:
• a profound autistic withdrawal;
• an obsessive desire for the preservation of sameness;
• a good rote memory;
• an intelligent and pensive expression;
• mutism, or language without real communicative intent;
• oversensitivity to stimuli;
• a skilful relationship to objects.
Kanner explained that he referred to the work of Bleuler (1911) when choosing the word ‘autism’ to describe what he saw. Bleuler used the term to describe a withdrawal from previous participation, whereas the children Kanner described had never engaged in social interaction.
Triad of impairments
As the information provided by Kanner's observations on the nature of autism became more widely known, more children were referred for diagnosis. Sets of criteria and checklists were developed to aid diagnosis. As more children were seen, it became clear that Kanner had recognised only one small group of children who fitted his particular criteria. The list of Kanner's defining features was felt to be too limiting by those who were involved in diagnosis. There were children for whom it was felt that a diagnosis of autism would be a useful descriptor yet who did not fit exactly into the criteria outlined by Kanner.
In 1979 Lorna Wing and Judith Gould carried out a study in the London Borough of Camberwell, looking at all children under 15 who had any kind of physical or learning disability or abnormality of behaviour, however mild or severe. Examining the findings of their study, they were able to pinpoint the social nature of the difficulties and identified what they described as the ‘Autism Triad’ of impairments:
•impairment of social interaction;
•impairment of social communication;
•impairment of social imagination.
Autism spectrum
Wing and Gould identified a number of children with what they described as ‘Kanner's syndrome’, and a larger number who showed similarities to this group, but didn't fit Kanner's criteria exactly. Thus, in 1988 Wing went on to use the broader term ‘Autistic Continuum’ and later ‘Autistic Spectrum’ (Wing 1996).
The term ‘spectrum’ has been useful in allowing for a broad definition of autism based on the triad of impairments and has been described by Jordan (1999) as being most appropriate in facilitating educational approaches to autism. Intervention and treatment approaches for children anywhere within the spectrum of autism will share the same foundation.
Diagnostic criteria
Diagnosis of autism continues to be based on the interpretation of a child's observed and reported behaviours, which is not the most clear-cut diagnostic tool. Although it is recognised that autism can occur whatever the intellectual capacity, many of the children may also have an additional general learning difficulty. This adds to the difficulty in diagnosis, as it becomes increasingly difficult to separate out the effects of autism and the effects of profound and multiple difficulties.
Wing and Gould (1979) in the Camberwell study found that 60 per cent of the children with autism had severe learning difficulties, 25 per cent had moderate learning difficulties and 15 per cent were of average and above average intelligence.
There is acceptance now that autism is distinguished by the co-occurrence of the impairments in social interaction, social communication, social imagination, flexible thinking and play. Diagnostic criteria are agreed on the basis of the triad. The two major diagnostic instruments currently used by clinicians base their criteria on these three fundamental impairments, i.e. DSM IV (Diagnostic and Statistical Manual of Mental Disorders, 4th edition, American Psychiatric Association (APA) 1994) and ICD 10 (International Classification of Diseases, World Health Organization (WHO) 1992).
Numbers of children
There have been attempts to define the number of people with autism; the totals identified range from 5 per 10,000 of population to 91 per 10,000. This wide range of prevalence figures causes confusion if it is not looked at with care. Most studies suggest that between 4 and 6 per 10,000 can be classified as having ‘Kanner's autism’. The National Autistic Society (1997) suggests a prevalence figure of 91 per 10,000. This figure relates to the broadest definition of autism, including those with classic ‘Kanner's autism’, those who may best be described as having Asperger syndrome, together with those who have impairments within the triad, but do not fit into either Kanner's autism or Asperger syndrome.
All prevalence studies reflect Kanner's findings that boys outnumber girls in the autistic community. Ciadella and Mamelle (1989) suggest two boys to every one girl, while Lord and Schopler (1987) suggest the ratio is 5:1.
Causes
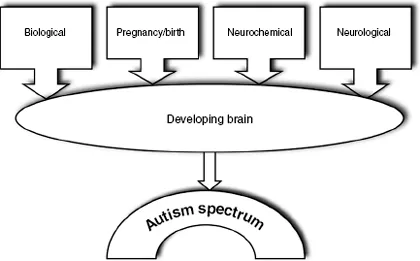
As yet the cause of autism is unknown. It is felt that there is not one single cause, rather a set of triggers, any one of which, if it occurs at a certain time within a chain of circumstances, can cause autism (see Figure 1.1).
1.1 Factors which trigger conditions on the autism spectrum
Until there is more information as to the causes of autism it may be more useful to specify the functions which are affected and look for ways in which intervention may help at this stage.
Summary
•Child psychiatrist Leo Kanner first described autism in 1943.
•Autism is regarded as a physical disorder of the brain which causes a lifelong developmental disability.
•Estimates of the prevalence of autism range from 5 per 10,000 of population to 91 per 10,000.
•Boys are more likely to be affected than girls, with suggested ratios ranging from 2:1 to 13:1.
•Autism affects children right across the ability range.
![]()
CHAPTER 2
Assessment and diagnosis
Key features of autism
Autism is characterised by significant impairments in three main areas of development. Typical features which present in the early years include the following.
1 Social interaction
The young child on the autism spectrum:
•cannot make sense of people, and may find them frighteningly unpredictable;
•seems to relate better to objects than to people;
•may only tolerate approaches from very familiar people;
•may only make approaches to people he knows well;
•may seem to use people only as a means to an end – perhaps to obtain something out of their own reach (Richard preferred to help himself to food from the kitchen, dragging a chair to help him climb up and open the cupboard. Only if this strategy failed would he pull his Mum into the kitchen and ‘throw’ her hand up towards the item he wanted – all without vocalisation or eye contact);
•is usually unaware of simple social rules and conventions.
2 Social communication
The young child on the autism spectrum:
•is slow to develop speech, and may not develop speech at all;
•if he uses words, often uses them out of context and without communicative intent;
•may echo the words of others – straight away, or later (Curtis spoke with an American accent, despite having English parents – he'd acquired most of his language from repeatedly watching cartoon videos);
•may use words and then ‘lose’ them (At 18 months Lewis was shouting ‘Daddy’ up the stairs, and had around 20 words in his vocabulary. By the ...