An international team of contributors come together to present all clinically relevant aspects of leukemias, lymphomas, and myelomas. Using clear terminology, the book discusses salient features, diagnostic procedures, prognosis, and treatments for these cancers.Following on the successful steps of the first edition, this Second Edition covers: various types of leukemias, lymphomas, and myelomas utilizing stem cell transplantation side-effects of various treatments future prospects for leukemia, lymphoma, and myeloma targeted therapies and history of the cancers information and support sources for patients
Frequently asked questions
How do I cancel my subscription?
Simply head over to the account section in settings and click on “Cancel Subscription” - it’s as simple as that. After you cancel, your membership will stay active for the remainder of the time you’ve paid for. Learn more here.
Can/how do I download books?
At the moment all of our mobile-responsive ePub books are available to download via the app. Most of our PDFs are also available to download and we're working on making the final remaining ones downloadable now. Learn more here.
What is the difference between the pricing plans?
Both plans give you full access to the library and all of Perlego’s features. The only differences are the price and subscription period: With the annual plan you’ll save around 30% compared to 12 months on the monthly plan.
What is Perlego?
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1 million books across 1000+ topics, we’ve got you covered! Learn more here.
Do you support text-to-speech?
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more here.
Is Understanding Leukemias, Lymphomas and Myelomas an online PDF/ePUB?
Yes, you can access Understanding Leukemias, Lymphomas and Myelomas by Tariq I. Mughal in PDF and/or ePUB format, as well as other popular books in Médecine & Oncologie. We have over one million books available in our catalogue for you to explore.
The simplest definition of hematological cancers is that they are cancers which arise from a single blood cell. Since all blood cells are produced by a process called hematopoiesis (“heme” comes from the Greek word haema or “α
μα” for blood and “ποíηο
” or poiesis means creation or formation), cancers such as leukemias, lymphomas, and myelomas are often referred to as blood cancers. The cancer type usually refers to the organ or the specific type of cell where cancer originates. To distinguish blood cancer from other forms of cancers, they are sometimes referred to as “liquid tumors” since they typically do not form lumps or masses (“tumors”). In contrast, cancers arising from all other cells, which typically form masses, are called “solid tumors.”
Leukemias, lymphomas, and myelomas are not single diseases, but rather encompass a large number of subtypes with a broad range of natural histories, ranging from those which remain indolent for long periods to those that grow rapidly and can prove fatal very quickly if untreated. In order to understand them, it is useful to know something about cancer in general.
The word “crab” (Greek καρκívoϛ, or “cancer” in Latin) was introduced by Galen of Pergamon, a Greek physician to the Roman Emperor Marcus Aurelius, sometime between AD 129 and 216. Cancer appears to have been present since time immemorial, perhaps even before the evolution of man, as it had been noted in bones of dinosaurs and our ancestors Pithecanthropus erectus. It was first recognized by Hippocrates, on the Greek island of Kos, ca. 460 to 370 BC. In AD 30, Aurelius Celsus, a layman, remarkably described the uncontrolled growth of cancer cells.
Cancer is a common disease today, and in developed countries approximately 20% of the population, and considerably more in developing countries, die of cancer. Sadly, it is anticipated that cancers will become even more common in the future. The WHO predicts that by the year 2020, it is likely that a staggering one in two of the global population will develop cancer during their lifetime. This striking increase is mainly due to the increasing age of the population worldwide. Put very simply this means that with the predicted global population of 8 billion in 2020, over 20 million new cancer patients will be diagnosed each year.
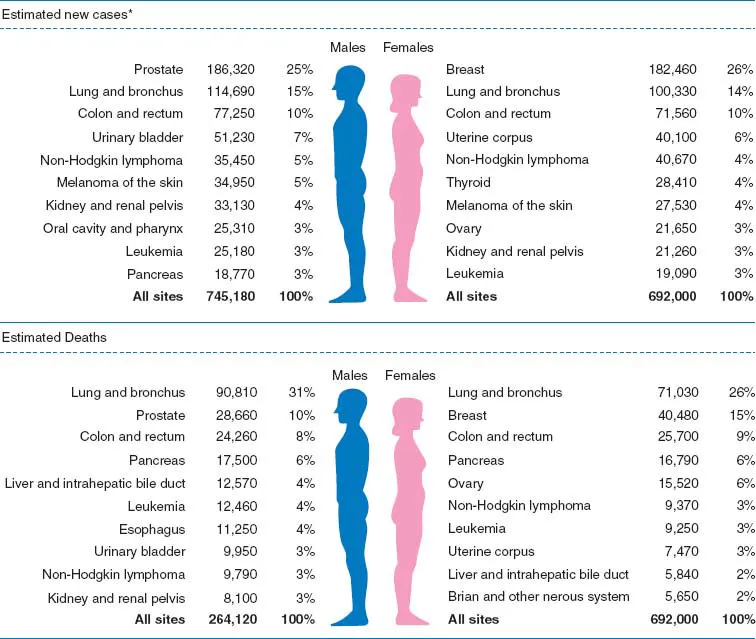
Although enormous advances have been made in the treatment of an increasing number of cancers, in particular blood cancers, testicular cancers, and several other rare cancers, the treatment of the vast majority remains very unsatisfactory. For example, in lung cancer, which is probably the most common type of cancer in the world today, fewer than 10% of patients are actually “cured” (defined as being completely free of the cancer in the long term). A report from the U.S. American Cancer Society, based on data collated by the National Center for Health Statistics, National Cancer Institute, Centers for Disease Control and Prevention, and the North American Association of Central Cancer Registries, analyzing data on all deaths from cancer and from cancer at specific sites, as well as on deaths due to cancer according to age, race, and sex, for the years 1994 to 2004 for women and 1995 to 2004 for men, revealed that although much progress has been made, there is still largely a disappointing effect of cancer treatments on mortality (Figs. 1.1 and 1.2). It suggested that the most promising approach was to have a firm commitment to prevention, with a concomitant “rebalancing” of the focus and funding of cancer research. This does not mean that most cancers are invariably fatal, since major progress has been made in many different types of cancers, which in some cases allows some patients to live to their normal life expectancies even though they still have a cancer, which effectively is managed as chronic disease.
Our task in providing an optimal treatment for all cancer patients is therefore daunting. The advances in our knowledge of the basis of how cancer arises promise to improve our ability to categorize, diagnose, and treat cancer. Globally, many governments and other organizations are firmly committed to improving the outcomes for cancer patients, and large financial investments are being made in cancer research, targeted prevention programs, cancer screening, and other related steps; without further improvements, over 12 million of the projected 20 million patients will die from the effects of their cancers.
Cancer patients are among the most significant recipients of healthcare spending in the United States, with the National Institutes of Health estimating its costs in 2002 at $171.6 billion, of which nearly $61 billion was attributed to direct medical costs; it has been estimated that these costs will be at least tripled, if not quadrupled, by 2010. On that note it was gratifying to witness U.S. President Barak Obama’s March 2009 address to Congress, in which he promised to launch new efforts (by increasing funding for cancer research) to find a cure for cancer in “our time.” Several global reports, such as the American Society of Clinical Oncology’s December 2009 Special report and others, show declines for overall cancer death rates and for many of the top 15 cancers, along with improved survival rates, reflecting progress in the prevention, early detection, and treatment of cancer. However, there were considerable ethnic and geographical variations, suggesting that not all members of the U.S. population benefited equally from such advances. Sadly, this is probably true for most other parts of the world, where considerably smaller improvements have occurred, even in developed countries like the United Kingdom.
Figure 1.1 Ten leading cancer types for the estimated new cancer cases and deaths, by sex, U.S.A., 2008. *Excludes basal and squamous cell skin cancers and in situ carcinoma except urinary bladder. Estimates are rounded to the nearest 10. Source: Used with permission from Jemal A, Siegel R, Ward E, et al. CA Cancer J Clin 2008; 58: 71–96.
WHAT HAPPENS IN CANCER?
The past few decades have witnessed remarkable insights into what happens in cancer. Historically, at least since Roman times, it was believed that cancer could run in families; the first reported cases of familial cancers in the medical literature (in this case, breast cancer) were described by Paul Broca in Paris in 1866. In 1914, Theodor Boveri suggested that an aberration in the genes (a gene is the basic unit of inheritance) might be responsible for the origin of cancer. Cancer is now firmly recognized as a genetic disease since genetic changes occur when a normal cell is transformed into a cancer cell; these changes only occur in the cancer cells and are not present in normal cells. The word genetic is used here to imply that genes are involved and does not mean that there is any inherited predisposition. In some cases, genetic predisposition can be inherited, although in the vast majority of cancers there is no known inherited predisposition.
Recent significant insights into the origins of familial cancers have helped define many hereditary cancers and have helped understand the unique abnormalities in cell function, which paved the way to developing genetic testing. Genetic testing allows patients and family members to make better-informed assessments of their individual cancer risk, which in turn allows them and their physicians to make rational decisions about potential preventive and surveillance options. In simple terms, cancer cells carry certain characteristics in their genetic makeup that are unique in that they enable genetic changes to be passed from one cell to another (horizontally, somatically) as opposed to the usual inherited changes that are carried from parent to child (vertically, germ-line). Alterations (cancer-specific mutations) in genes, inherited or acquired, pave the way for a normal cell to become cancerous (or neoplastic or malignant, in the parlance of cancer medicine). This is exemplified by several observations, including those of Mel Greaves and his colleagues in London. They investigated whether a leukemia-specific abnormality arises in infants who develop acute leukemia (in this case, acute lymphoblastic leukemia) prenatally (prior to birth). By means of an elegant analysis of neonatal Guthrie blood spot cards (see “Glossary”) for children aged between two and five years, who had newly diagnosed leukemia, they were able to confirm that some childhood leukemias do indeed start before birth. Studies in identical twins show, however, that the first event is not by itself sufficient for the clinical development of leukemia and that additional postnatal genetic events are required, lending support to the notion of the sequential nature of the acquisition of abnormal (pathological) genes over a certain time period.
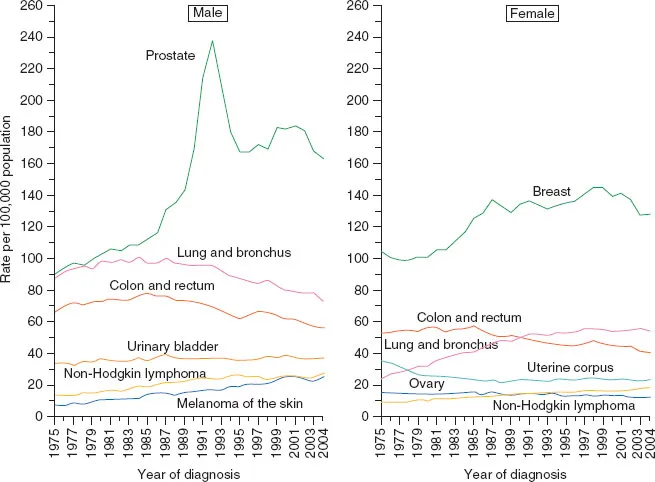
Figure 1.2 Annual age-adjusted cancer incidence rates for selected cancers by sex, U.S.A., 1975 to 2004. (Rates are age-adjusted to the 2000 U.S. standard population and adjusted for delays in reporting.) Source: Used with permission from Surveillance, Epidemiology, and End results Program (www.seer.cancer.gov). Delay-adjusted incidence database: “SEER incidence delay-adjusted rates, nine registries, 1975 to 2004.” National Cancer Institute, DCCPS, Surveillance Research Program. From Jemal A, Siegel R, Ward E, et al. CA Cancer J Clin 2008; 58: 71–96.
MOLECULAR BASIS OF CANCER
A cell is the smallest single living unit and there are about 1014 (or one hundred trillion) cells in the human body. There are many different types of cells. They have a surface membrane (“skin”), which is vital for the recognition and behavioral control of the cell; cytoplasm (“pulp”) that harbors the “cytoskeleton,” which is made up of a network of microfilaments in microtubules and influences the cell’s shape, motility, adhesion, and division; and a nucleus (“pip”) that can be thought of as the cell’s brain or command center. Figure 1.3 shows an electron micrograph of a cell.
Figure 1.3 An electron micrograph of a cell. Source: Courtesy of Dr. Brian Eyden.
The cell surface is composed mainly of a flexible lipid (“fatty”) structure in which a large number of complex proteins “float.” These proteins have external domains, which can be recognized by the immune system from outside the cell. Internally many of these molecules connect with multiple pathways (known as signaling pathways) that are part of an elaborate communications system which permits us to perceive, integrate, and respond appropriately to local, environmental, and behavioral stimuli. Figure 1.4A is a simplified depiction of a cell’s signaling pathways; Fig. 1.4B depicts some of the signaling pathways known in chronic myeloid leukemia (the complexity of these pathways, as the knowledge unfolded in the last decade of the last century of the last millennium, often reminded specialists of the quotation from William Shakespeare’s Hamlet, Act II, Scene II: “Though this is madness, there is method in it”). Many of the complex proteins on the cell surface also act as “pumps,” whereby they can regulate the intrusion/extrusion of materials to the cell. The cell surfaces also harbor “receptors,” which can send messages to the nucleus. For example, one of these critical receptors is the growth factor receptor, which can send signals for increased growth to the nucleus. Each specific molecule links only with its unique cognate receptor, like a key in a lock. Binding of appropriate proteins and related substances known as ligands to the receptors or other cell surface molecules induces conformational changes (known as signal transduction in molecular biology parlance) and generation of second messengers. These messengers, in turn, activate other factors (known as transcription factors) which act on the nucleus and affect cell growth, survival, and function. These are some of the basic materials and processes that are important for the highly coordinated, integrated, and orderly function of the human body. We discuss the contents of the nucleus, which...