- 152 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Radiology Technologist's Handbook to Surgical Procedures
About this book
In the past several years, the rapid development of sophisticated imaging modalities has made radiology the fastest growing specialty in medicine. It is important for the radiologic technologist to keep pace with technology's advancements.
The influx of freestanding outpatient facilities and the demands of insurance companies, HMOs and third party reimbursement have brought about change. Medical facilities have begun to call upon nurses, surgical technicians, and other non-radiologic personnel to assist with patient positioning during surgical procedures requiring imaging-creating a need for a concise, how-to guide to performing surgical procedures.
The Radiology Technologist's Handbook to Surgical Procedures provides a quick reference for using fluoroscopic and x-ray equipment during surgical procedures. This book includes detailed descriptions and photographs taken in actual clinical settings.
By using this manual as a foundation, the radiologic technologist will be able to master many of the operating room x-ray procedures.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Fluoroscopic Examinations
1. FEMORAL NAILING
(AP POSITION)
PATIENT POSITION: Patient will be in lateral position with affected femur up and slightly forward.
C-ARM POSITION: C-arm will enter facing patient. Rotate c-arm underneath the table to the ap projections. Ensure that c-arm is perpendicular to femur.
Notes: When moving from ap to lateral position, make sure not to bump instrumentation.
Position c-arm viewing cart at feet of patient with the doctor standing posterior to the patient.
Create distance and magnify image when creating round holes for distal locking screws.
During reaming, obtain true lateral of knee by tilting and rotating c-arm.
Position the c-arm to view reamers crossing fracture site.
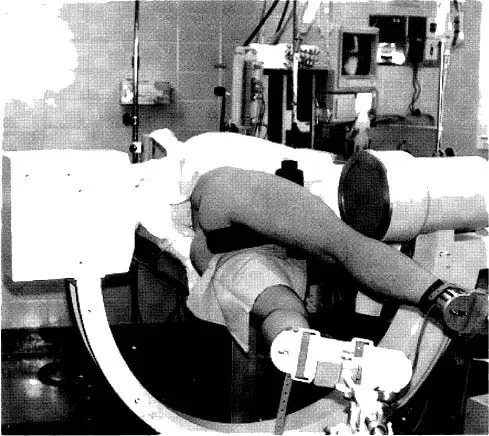
Figure 1.1 C-arm in ap projection of hip.

Figure 1.2 C-arm image of ap hip with nail inserted.
2. FEMORAL NAILING
(LATERAL POSITION)
PATIENT POSITION: Patient will be in lateral position with affected femur up and slightly forward.
C-ARM POSITION: C-arm will enter facing patient. Rotate c-arm 10 to 15 degrees over top of patient. Tilt c-arm 5 to 10 degrees toward head of femur.
This view, called the Winquist View, is used to throw the unaffected femur out of view, to elongate the femoral neck for true lateral viewing of starting position and to check anterior and posterior position.
Notes: When moving from ap to lateral position, make sure not to bump instrumentation.
Position c-arm viewing cart at feet of patient.
Doctor will stand posterior to patient.
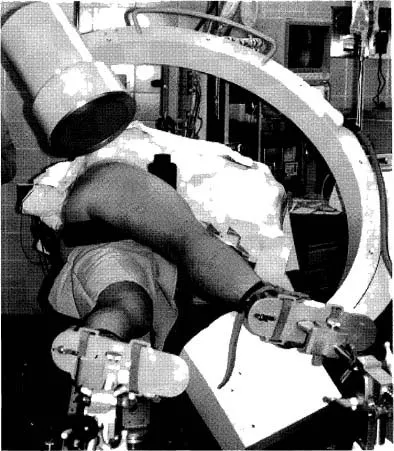
Figure 2.1 C-arm in lateral projection with Winquist tilt view.
Figure 2.2 C-arm image of lateral hip with starting auld in place.
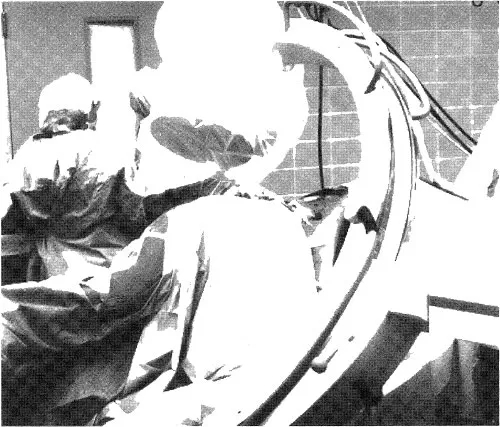
Figure 2.3 The c-arm is in the Winquist view, which is best utilized to check anterior and posterior positions in relationship to the femoral shaft. The c-arm is rotated over the top and tilted to elongate the femur.
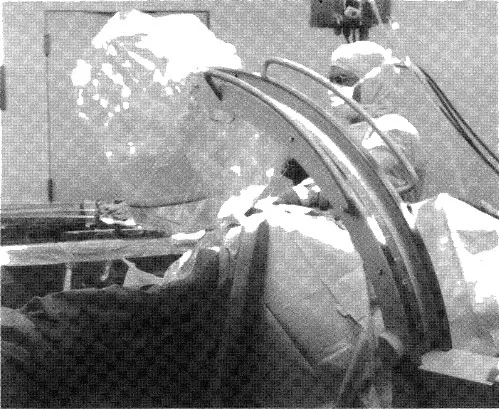
Figure 2.4 The c-arm in a true lateral view in relationship to femur position. The c-arm is tilted to align with the femur. This will give a better indication of fracture alignment and reamer size.
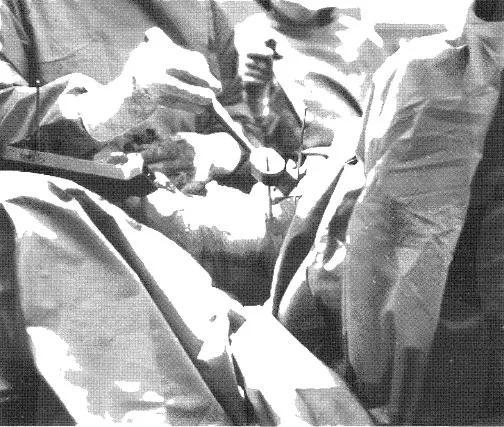
Figure 2.5 During distal targeting for femoral nail, raise the c-arm away from the knee to enlarge the hole and create working space. Use the magnify button on the c-arm if available.

Figure 2.6 Incorrect hole alignment. Note how hole is oblong.
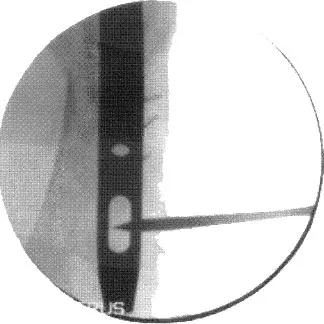
Figure 2.7 Correct hole alignment. Note that hole is now rounded.
3. SUPRACONDYLAR FEMORAL NAIL
(AP VIEW)
PATIENT POSITION: Patient will be supine with the affected knee slightly bent on radiolucent table.
C-ARM POSITION: C-arm will enter perpendicular to patient and in the ap position.
Notes: Ensure underneath clearance allows for movement from the knee to the hip.
C-arm may have to be rotated over or backward to create a true ap view.
Tilt c-arm to open joint space of knee for starting point.

Figure 3.1 C-arm in ap projection of distal femur.
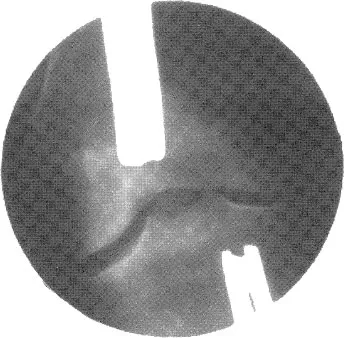
Figure 3.2 X-ray image of distal femur.
2323__...Table of contents
- Cover
- Title Page
- Copyright Page
- Table of Contents
- PART I: Fluoroscopic Examinations
- Part II: Intra-Operative Examinations
- Appendix: Glossary of Terms
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Radiology Technologist's Handbook to Surgical Procedures by AnthonyC Anderson in PDF and/or ePUB format, as well as other popular books in Medicine & Forensic Science. We have over 1.5 million books available in our catalogue for you to explore.