This book is an introduction to audiology for those who have little or no knowledge of the subject. It introduces basic aspects of audiology in a clear and accessible way. This initial knowledge is then developed to a depth which allows the reader to access more specialised journals and textbooks.
eBook - ePub
Audiology
An Introduction for Teachers & Other Professionals
- 128 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
The Ear and How it Works
Anatomy and physiology of the ear
The ear can be divided into three parts. The outer ear, the middle ear and inner ear (Figure 1.1).
The outer ear
The outer ear comprises:
- the pinna or auricle;
- the ear canal or external auditory meatus;
- the ear drum or tympanic membrane.
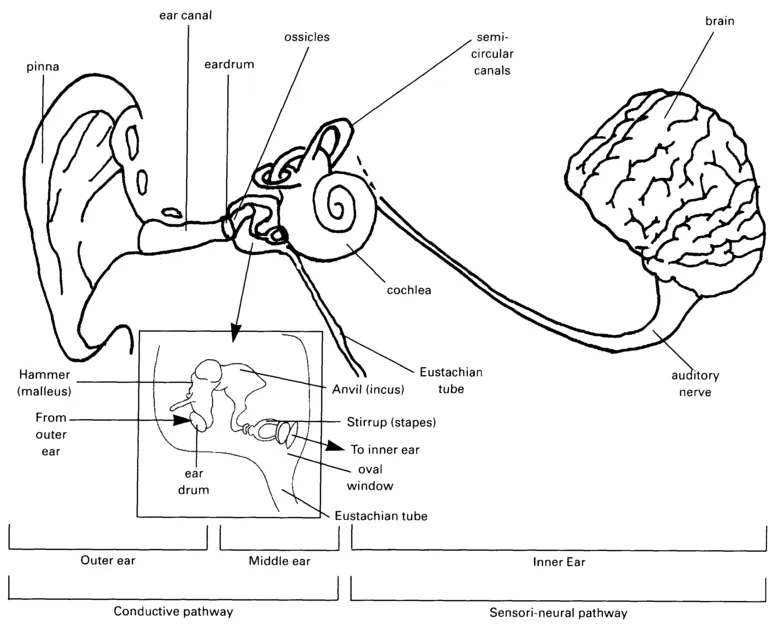
Figure 1.1 The complete hearing system (after Tate 1994)
The pinna or auricle is a structure of pliable cartilage with a tight covering of skin. It is a complex shape designed to collect sound waves, particularly from a forward direction, and funnel them into the ear canal and to the ear drum. The pinna enhances sound reception by about 5dB and assists with the localisation of sound.
The ear canal, or external auditory meatus, is a tube approximately 2.5 cm long which is closed at the inner end by the ear drum or tympanic membrane. The outer third of the ear canal is composed of cartilage, which is continuous from the pinna. This part of the ear canal contains ceruminous glands. These secrete cerumen or wax which helps to protect the ear canal and to moisturise the air in the canal. Wax, which is a mixture of the secretions of sebaceous and sweat glands, mixes with the skin debris which collects in the ear, and migrates naturally outwards, eventually coming out of the ear as a brown moist secretion. Wax is water resistant and inhibits bacterial growth thus protecting the ear from infection. Wax is a natural substance and should not normally be artificially cleaned out of the ear canal.
The inner two thirds of the canal are composed of bone lined with skin, which becomes very thin in the deeper parts of the canal.
The ear drum or tympanic membrane is the membrane found at the end of the canal, separating the outer ear from the middle ear. It is composed of three layers:
- the outer layer is a skin or epithelial layer;
- the middle layer is a fibrous layer;
- the inner layer is a mucosal layer.
The ear drum itself is divided into an upper and a lower section. The upper section is the smaller. It has no fibrous layer and is called the pars flaccida. The lower and larger portion of the membrane is called the pars tensa.
The ear drum vibrates in response to sound waves (acoustic energy) funnelled down the ear canal. These vibrations pass from the ear drum to the bones in the middle ear. The ear drum changes, or transduces, the acoustic energy into mechanical energy in the middle ear.
The middle ear
The middle ear, Figure 1.1, is an air filled cavity beyond the ear drum. A chain of three bones, called ossicles, is supported by ligaments and muscles and bridges the middle ear cavity. The three bones in the ossicular chain serve to link the outer ear to the inner ear. They have a vital function in the transference of sound energy from the outer ear to the inner ear and can increase the intensity of the sound by about 28 dB.
The chain consists of the malleus (hammer) which has a handle and a head. The handle is attached to the ear drum and can be seen though the ear drum by means of an otoscope. The head of the malleus is attached to the incus (anvil) by a joint. The anvil makes contact with the head of the stapes (stirrup). The footplate of the stapes is attached to the oval window, which is the entrance to the inner ear.
Sound passes most effectively through the middle ear when the air pressure in the middle ear is equal to the atmospheric pressure. This pressure equalisation is maintained by the Eustachian tube.
The Eustachian tube is about 3.5 cm long and runs in an inward and downward direction, from the middle ear, opening into the nasopharynx or throat. The function of the Eustachian tube is to balance the air pressure in the middle ear and also to drain the middle ear of any gathering fluid or mucus.
The middle ear also serves to protect the delicate inner ear structures from any potentially damaging noises. In response to loud sounds, especially low frequency (see Chapter 2), the middle ear muscles contract, causing the ossicular chain to stiffen and so transfer sound less effectively.
The middle ear ends at the oval and round windows, which separate the middle ear from the inner ear. These windows are membrane-covered holes in the bony wall of the cochlea.
The inner ear
The inner ear consists of all those parts of the auditory system beyond the middle ear. Sound waves pass through the oval window to the cochlea where they are converted into electrical signals, which travel along the nerve or neural pathways to the auditory centre of brain. The inner ear is concerned with both hearing and with balance. The cochlea is concerned with hearing while the three semi-circular canals are concerned with balance and are part of the vestibular system. The cochlea and the semi-circular canals make up a fluid filled cavity, which is set in the petrous portion of the skull.
The cochlea
The cochlea looks rather like a snail shell, has two and a half coils and is about the size of a pea. A cross-section of the cochlea (see Figure 1.2), allows us to see that the cochlea has three fluid-filled 'galleries'. These are:
- the scala media,
- the scala vestibuli and
- the scala tympani.
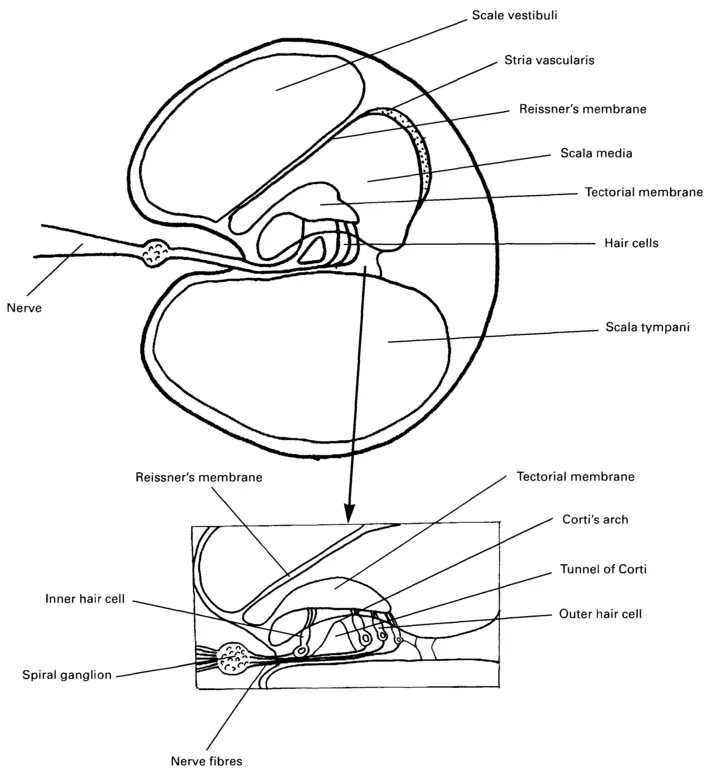
Figure 1.2 Cross-section of the cochlea (after Tate 1994)
The Organ of Corti lies in the central gallery of the cochlea. It consists of rows of hair cells served by nerve fibres. The hair cells are responsible for the transduction of mechanical vibrations received from the middle ear, into electrical impulses. The sound waves travel along the basilar membrane and 'deform' it. Because of the movement, nerve impulses are sent along the nerve fibres. The nerve fibres join to form the auditory nerve, which is part of the eighth cranial nerve. The cochlea is the site where sounds are first analysed into their component frequencies. Different parts of the basilar membrane are sensitive to different frequencies of the sound spectrum (like a piano keyboard). The base of the cochlea is sensitive to high frequency sound waves and the apex of the cochlea is sensitive to low frequency sound waves. All sound waves must travel across the base of the cochlea and maximum 'wear and tear' occurs in this area. Therefore high frequency hearing losses are the most common.
The auditory nerve and brain
The auditory nerve carries the signal to the hearing centres of the brain. The brain interprets frequency according to the part of the cochlea from which the nerve impulses are sent and the intensity according to the number of nerve impulses received.
The area of the brain that is primarily involved in decoding sensory information is the cerebral cortex. Signals from each ear are sent to both left and right hemispheres of the brain but most information is projected to the opposite side of the body. Thus neurons from the left cochlea project predominantly to the right cortex and vice versa. At a functional level, the cortical auditory regions in the left and right hemispheres have different specialisations. The left hemisphere is specialised for language processing (Binder et al. 1996) and the right hemisphere for processing music (Penhune et al. 1999).
Aetiology: types and causes of deafness
Types of deafness
Audiologically the ear can be divided into conductive and sensorineural pathways in relation to the transmission of sound energy. The type of deafness is largely related to the place in the hearing system where the cause of deafness is situated.
- Conductive hearing loss is deafness resulting from any malfunction or abnormality which prevents or reduces the conduction of sound waves through the outer or middle ear to the oval window of the inner ear.
- Sensori-neural hearing loss or 'nerve' deafness is hearing loss that occurs in the inner ear, i.e. the cochlea, the auditory nerve, the auditory pathway or the hearing centres of the brain. This prevents, reduces and distorts the sounds reaching the auditory cortex.
- Mixed hearing loss describes the presence of sensori-neural deafness with some conductive deafness in addition.
- Unilateral or monaural hearing loss is deafness that is apparent in one ear only. It may be conductive or sensori-neural or mixed. The child can hear well in one ear but may have difficulties in noisy surroundings and with locating the direction of sound (see later in this chapter).
Causes of deafness
Most causes of deafness in children fall into three categories:
- hereditary (congenital);
- peri-natal (that which occurs around the birth);
- acquired (occurring during a child's lifetime).
These can affect the conductive pathway, the sensori-neural pathway, or both.
Conductive hearing loss
Causes of conductive hearing loss
Hereditary conductive hearing loss is largely caused by:
- Anatomical abnormalities - these arise in the womb as the ear is developing and can include an absence of the outer ear, atresia (occlusion or closure of the ear canal) and the absence of ossicles.
Peri-natal conductive hearing loss is largely caused by:
- Fluid and debris in the ear canal, which is usually treatable.
Acquired conductive hearing loss is largely caused by:
- Otitis media or inflammation of the middle ear. This is one of the most common disorders in children. The most usual cause is the loss of eustachian tube function, through upper respiratory tract infections (throat and nose infections) impairing the function of the middle ear. This condition, also called glue ear, is discussed further in the following section.
- Foreign bodies - children sometimes push small items, for example beads, into their ears. If these block the ear canal, they will cause some degree of deafness.
- Otitis externa or inflammation of the outer ear. If the ear canal swells or if there is discharge, this may also cause hearing loss. The whole canal can be affected or a localised area. In either case the ear canal is very tender.
- Impacted wax. Wax may accumulate and turn brown and hard in the ear canal. It will cause hearing loss if it blocks the ear canal. This deafness may be accompanied by a 'buzzing' tinnitus.
- Otosclerosis is a condition in which the movement of the stapes is restricted by an abnormal growth of bone in the ossicular chain. (Otosclerosis is a hereditary condition which is not present at birth but which develops later in life).
- Stenosis is a closure or narrowing of the ear canal. (Atresia is similar but present at birth).
Glue ear (Otitis Media)
The most common cause of conductive hearing loss is otitis media, commonly known as 'glue ear'. This is a prevalent condition in children under eight years old. About 15-20 per cent of children in the two to five year age range will have 'glue ear' at any one time. Glue ear gives rise to fluctuating hearing loss, which is largely a passing condition but it is important to realise that when it is present it can significantly affect children's hearing at a crucial time in their linguistic development.
Otitis media occurs when ...
Table of contents
- Cover
- Title
- Copyright
- Contents
- Foreword
- Acknowledgements
- Introduction
- Glossary
- 1 The Ear and How it Works
- 2 The Physics of Hearing
- 3 Assessment of Hearing Loss
- 4 Amplification Systems
- 5 The Acoustic Environment
- 6 Systems in the Classroom
- 7 Cochlear Implants
- 8 Management and Maintenance of Hearing Aids
- 9 Assessing the Benefits of Hearing Aids
- 10 Teachers' Roles and Responsibilities
- 11 Developing Spoken Language
- Appendix 1: Audiological descriptors
- Appendix 2: Checking hearing aids
- Appendix 3: Checking radio hearing aids
- Appendix 4: General instructions for using a test box
- References
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Audiology by Mary Anne Maltby,Pamela Knight in PDF and/or ePUB format, as well as other popular books in Education & Education General. We have over 1.5 million books available in our catalogue for you to explore.