Please Help Me With This Family is based on the premise that it is generally useful to expand the therapeutic system when it is not working. By calling in additional resources when therapy reaches an impasse, the therapist is giving two strong messages to stuck families-(1)the admission of the failure of the present system to grow beyond the impasse, and (2) a model of creativity in recruiting resources to improve chances of success. Often, the resources in the large system hold the keys to uncovering and correcting troublesome relationships and behaviors in the smaller system. Please Help Me With This Family is divided into four major sections, each illustrating unique approaches and methods for unlocking resources in family and therapeutic systems. The first section opens with a comprehensive review of the theoretical roots of family therapy consultation, followed by a discussion of the different faces of consultation around the world; a detailed case study of an anorectic family in which Maurizio Andolfi successfully provokes a therapeutic impasse; and to which Carl Whitaker provides fascinating insights into his role as a consultant. Section II discusses the variety of consultative resources available in the client system and how best to harness them. Chapters cover using the child as consultant; using family of origin and friends as resources; and the use of consultation in treating addictions. Using colleagues as consultants is the focus of the third section. Consultation has the advantage over cotherapy and supervision of requiring only a brief, cost?effective relationship. Chapters discuss how therapists can avoid replicating errors by working closely with the client's previous therapist: an eco?systemic approach with chronic pain sufferers that involves medical, family, and community systems in Israel; using consultation to evaluate therapy; the creative?preventive possibilities inherent in collegial consultation; how a family therapist and school system personnel can be mutually helpful with a conjoint problem; and a consultation that focuses on the position of the therapist rather than on the client system. Finally, Section IV addresses consultation as a valuable form of professional development. It explores the importance of timing when using a consultant; the effects on five therapists of live case demonstrations with Maurizio Andolfi as consultant; and consultation to correct gender prejudice. Contributors to this volume include Vincenzo F. DiNicola, Elizabeth Ridgely, Joseph Simons, David Keith, Jim Guinan, William Jones, Lars Brok, Joel Elizur, Sara B. Jutoran, Noga Rubinstein?Nabarro, Bob Wendt, Audrey Ellenwood, Peter Liggett, Marsha Purvis, Mary Hotvedt, and Marcella de Nichilo. Students and clinicians who wish to practice consulting as well as family therapists who want to learn creative approaches to handling the dilemmas that arise in therapy will find Please Help Me With This Family to be an incomparable resource.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
ELICITING COLLEGIAL RESOURCES FROM THE THERAPIST'S SYSTEM
9
The Referrer: Colleague, Client, or Pain in the Ass
____________________
Lars Brok and Rick A. Pluut
A referral to another therapist during an existing therapy can be viewed as a request for help by the referring therapist. The need for a referral occurs when the referrer feels unsure of his/her role in the therapeutic process. The referring relationship depends upon the stage of the therapeutic process at the moment of referral, the positions of the referring and consulting therapist in the work system, and the professional relationship between the referring therapist and the consulting therapist. The referring relationship can be a very effective one if well defined and collaborative; however, problems arise when this relationship is not well defined nor collegial. This results in what I call a “pain-in-the-ass” relationship.
Referral is a common procedure when therapists treat patients and patient systems for psychiatric problems. I have responded to approximately 200 referrals per year in the 12 years that I have worked on the admission ward and out-patient clinic of a general psychiatric hospital in the Netherlands. With most referrals, the referred patient or patient system has been in treatment for a considerable time with the referring therapist. Such referrals will be discussed in this chapter.
THE THERAPEUTIC PROCESS BEFORE REFERRAL
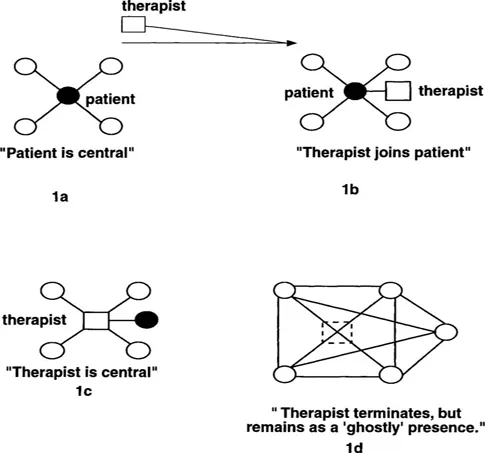
Since the timing of the referral in the therapeutic process needs to be carefully considered, I will briefly describe the phases of the therapeutic process in the original therapy system before any referral is made. These phases are contingent upon the various positions of the original therapist in the therapeutic system. To clarify these phases, I have further developed the diagrams of Andolfi, Angelo, Menghi, and Nicolo-Corigliano (1983, p. 83) and Andolfi, Angelo, and de Nichilo (1989, p. 144) regarding the therapeutic process (see Figure 1).
Figure 1a represents the situation before the onset of the therapy. The patient is central in the family (system) and is involved in every stressful relational triangle in the system (Andolfi, Angelo & de Nichilo 1989, p. 144).
The Wilson family wanted to commit their 15-year-old son who had been “unmanageable since he was two years old.” The parents told us that all conflicts between them were about this boy and that his mother feared to leave him home alone. His sister blamed her poor relationship with her mother on her brother because he occupied all of her attention. All agreed that the 15-year-old boy “ruled” the family.
Figure 1b represents the formation of the first phase of the therapeutic system. The therapist obtains a central position in the system by linking with the patient's symptoms. The therapist enters the system by acknowledging and provoking the centrality and, perhaps, the logic of the symptomatology.
In the first session with the Wilson family, the therapist put the son on a throne (made by a chair on top of a table) and asked the family to discuss the pros and cons of this heavy job the son had as “ ruler.” At the end of the session, the therapist asked the father if he wanted to overthrow the government and help his son abdicate the throne. The father agreed. The therapist told him that he would give him a task that would help him, but first he had to be sure that the father was stronger than the son. He asked the father and son to engage in an arm wrestle. Father and son fought with great pleasure and father won easily.
Figure 1c illustrates the therapist's substitution of him/herself for the patient's centrality in the therapeutic system. In this phase, problems other than the patient's symptoms may come up for discussion and family members may adopt less stereotypical roles in dealing with stressful events and problem resolution.
In the next session, the Wilsons brought up the theme of being overloaded. All family members felt overburdened in their own
Figure 1
way (the father at work, the mother at home, and the boy at school). The therapist became central by questioning each family member's motives to be overloaded. Issues concerning the parent's family of origin were discussed. The patient was no longer central and the symptoms soon disappeared.
In Figure 1d the therapy is officially ended. However, the therapist's (ghost) presence is still felt. If necessary, the therapist could be “materialized” again by the family (compare Andolfi, Angelo & de Nichilo, 1989).
We saw the Wilson parents for a follow-up consultation half-a-year later. This session took place on election day. The parents laughingly told us that they were determined that their coalition would remain in power and that the monarchy would have no chance of being reinstated. Thus, the therapist's influence remained in the family via the metaphor of the throne.
THE PROCESS OF REFERRAL
Many referrals occur when the therapist questions his/her role in the therapeutic process during a therapeutic impasse. Such referrals are often an appeal for help by the referrer rather than a request to take over the case (Zwanikken, 1979). Therefore, the consulting therapist should realize that this request for help/referral is an intervention by the therapist/ referrer in the therapeutic process. This intervention enlarges the therapeutic system by adding the consulting therapist.
The aim of the referring therapist is to restructure his/her position in the therapeutic system by creating an alternative reality: changing the interactional patterns, rules, values, and norms of the therapeutic system (Auerswald, 1985; Kantor & Neal, 1985). The role of the consulting therapist is central to the restructuring process in this system and is largely determined by the relationship with the referrer. This is similar to the relationship between the identified patient and the therapist (see Figure 1a) at the beginning of a therapy.
The referrer initiates this relationship by defining the problem. This problem definition is influenced by the role and position of the referrer in the therapeutic system, the phase of the therapeutic process at the time of the referral, and the referrer's perceptions of the consulting therapist's ability and ideology of therapy. It is important that the referrer clearly define the purpose of the referral at this time in the therapy. Thereafter, the referring and consulting therapists need to negotiate and mutually define their relationship.
The consulting therapist's goal is to develop a relationship that will provide additional information and help while maintaining the referrer's involvement. The following two types of relationships can accomplish this aim:
The collegial relationship. The referrer, in principle, remains in charge of the therapy and adopts a metaposition toward the consulting therapist. At the request of the referrer, the consulting therapist could provide a specific service within the framework of the ongoing therapy of the referrer. For example, the family therapist could ask a physician to prescribe medication to one of the family members in order to continue out-patient family therapy.
The consultative relationship. The referrer wants help to get unstuck and have the therapeutic process flow again. The consulting therapist could adopt a metaposition towards the referring therapist in the consultation process.
If the referring and consulting therapists do not clearly define their relationship, they can create what I call a “pain-in-the-ass” relationship. In this problematic relationship, the referring process often does not help create alternative roles in the therapeutic system, but rigidifies the already stereotypical roles.
THE PAIN-IN-THE-ASS RELATIONSHIP
Referrals that easily develop into a pain-in-the-ass relationship often start with a short message or phone call from the referrer to the consulting therapist:
Dear Colleague: I would like to refer Mrs. Holland to your admission ward with short notice. She has been on our ward for more than one year because of a borderline, personality disorder. A countertransference has developed with the nursing staff.
Dear Colleague: I would be grateful if you would take young man Stone in treatment. From nursery school and onwards, he has been in treatment with several therapists without success. I have seen his parents regularly for two years. The boy attended the sessions just a few times. His behavior was too difficult to handle in the sessions. The contacts with the parents were satisfying. The boy, however, remained unchanged. Probably a case of schizophrenia with mental retardation….
In each case, the referrer has circumvented the referral process by not including information about his/her position in the therapeutic system. The referrer has not taken partial responsibility for the continuance of the symptoms still existing in the therapeutic system. It is as if the consulting therapist has to meet a client system where a therapist does not even exist. Yet, the referrer gives clear advice about how to handle the case.
Selvini-Palazzoli, Boscolo, Cecchin, and Prata (1980) believed this type of referrer becomes an important family member, entangled in the family system. He/she becomes frustrated because all his/her efforts do not bring about any change while the family claims that he/she is indispensable for them. Although there is a referral, the referrer seems to obstruct the subsequent course of therapy.
Berg (1985) also described how these therapists not only refer, but dictate the treatment process. Like Selvini-Palazzoli, she emphasizes the unclarity of the referrer in the subsequent therapeutic system. Luyn and Vergouwen (1986) observed that such referrers wanted only to be relieved of the responsibility for their patients. The referrer views the consulting therapist as the rescuer. Peck, Howe, and Stackhouse (1978), on the contrary, interpret every application for referral as a request for consultation. They describe how quickly conflicts between the referring and consulting therapists can arise if one ignores the goals of the referrer.
A common feature noted by these authors is an undercurrent of irritation and complexity inherent in the referral process. I think that the basis for the irritation is the lack of communication between the referring and consulting therapists, which prevents a clear definition of their relationship.
Frequently, the following condition(s) obstruct the referral process:
The referrer is conspicuously uninterested in the consulting therapist.
The referrer presents a therapy plan that must be carried out by the consulting therapist. This plan or command, however, may include some of the following conditions:
a. unilaterally decided by the referrer;
b. very specific, although the referrer knows little about the prescribed treatment;
c. referrer does not take any responsibility for the proposed treatment plan;
d. the referrer could have done the treatment just as well;
e. the proposed treatment plan is incompatible with the frame of reference and/or possibilities of the consulting therapist.
The referrer allows one of the patients to make the first contact with the consulting therapist.
The referrer gives little information about the therapeutic process, particularly avoiding information about his/her position in the therapeutic system.
The referrer describes the patient(s) as unchangeable.
The referrer suddenly refers because of a change in his/her frame of reference. For example, a psychotherapist changes the definition of the problem to an individual, biological problem and refers the patient for pharmacological treatment.
The consulting therapist can also contribute to the evolvement of a pain-in-the-ass relationship with the referrer by responding to the referral with:
strikingly little interest in the referrer;
immediate and unconditional agreement to the referral;
premature and unsolicited advice for the referrer to carry out. This results in ideas that:
a. do not come about through consultation with the referrer;
b. are very specific, although the consulting therapist has little knowledge of the method involved;
c. include no co-responsibility of the consulting therapist for the implementation of the advice;
d. are not compatible with the capacities or theoretical frame of the referrer;
a hierarchical position that makes it difficult or impossible for the referrer to stay in charge of the therapy. For example, the referrer provides all of the extra efforts such as traveling and time commitments.
Occasionally the consulting therapist gives the impression that he/she would like to help the referrer, but without being involved in the referring process. Mostly, however, it is the referrer who “charmingly leaves” the therapeutic system. I agree with Selvini-Palazzoli et al. (1984) that this usually indicates that the referrer has become more like a family memb...
Table of contents
Cover
Half Title
Also by Maurizio Andolfi, M.D.
Full Title
Copyright
Dedication
Contents
Contributors
Foreword
Preface
Acknowledgments
I. AN OVERVIEW OF CONSULTATION WITH FAMILY THEORAPY SYSTEM
II. ELICITING RESOURCES FROM THE CLIENTS’ SYSTEM
III. ELICITING COLLEGIAL RESOURCES FROM THE THERAPIST’S SYSTEM
IV. CONSULTATION AS PROFESSIONAL DEVELOPMENT
Name Index
Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Please Help Me With This Family by Maurizio Andolfi, Russell Haber, Maurizio Andolfi,Russell Haber in PDF and/or ePUB format, as well as other popular books in Psychology & Education in Psychology. We have over 1.5 million books available in our catalogue for you to explore.