Complete Guide to Respiratory Care in Athletes introduces the respiratory system and its function during exercise. It considers the main respiratory conditions affecting athletes and delivers practical advice for the management of respiratory issues in athletic populations.
With contributions from leading international experts, the book discusses fundamental scientific principles and provides pragmatic 'hands-on' clinical guidance to enable practical application. Each chapter includes useful pedagogical features such as case studies and guides for carrying out assessments. The book covers wide a range of topics, including:
respiratory system function during exercise
impact of the environment on the upper and lower airways
asthma related issues in athletes
allergic rhinitis in athletes
exercise induced laryngeal obstruction
exercise induced dysfunctional breathing paterns
respiratory muscle training
role of screening for respiratory issues in athletes
assessing and dealing with respiratory infections in athletes.
This text is key reading for both newly qualified and established medical, scientific and therapy practitioners who are working with athletes with respiratory issues. It is also a valuable resource for students of sports medicine, sports therapy, and sport and exercise science courses.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
The anatomy and physiology of the respiratory system.
The physiology of how we breathe and what causes breathlessness.
How exercise influences the respiratory system.
Simple measures that can be used to evaluate the respiratory system and detect abnormal function.
An overview of cardiopulmonary exercise testing with focus on the respiratory response to exercise.
Introduction
The human respiratory system has evolved and adapted to ensure it serves its primary function; namely to transport the necessary oxygen required for energy generation at a cellular level and to remove waste products from this energy generation, primarily carbon dioxide. It is the latter, that is generally considered to dictate the overall functional behaviour of the respiratory system and during exercise mandates a response pattern acting to address metabolic requirements. Moreover, in highly trained athletic individuals the ability to surpass the exercise capacity of the sedentary individual places additional stress on the respiratory system and in some cases may be considered to limit exercise or impede exercise capacity (see Chapter 2). Overall however the pulmonary response patterns encountered are testament to how well the respiratory system adapts to these stresses, further demonstrating the evolutionary design of the human body to adapt to its surroundings.
The aim of this chapter is to introduce key aspects of the anatomy and physiology of the respiratory system in both untrained and trained (i.e. athletic) individuals, at rest and during exercise. The chapter also evaluates and details techniques that can be undertaken to assess the functional capability of the respiratory system to respond to the challenge of exercise.
Ventilation – how do we breathe?
Air enters the lungs via bulk flow due to a negative pressure being generated within the thoracic cage. This negative pressure is generated via contraction of the diaphragm, pulling the lungs downward and the intercostal muscles pulling the ribcage up and outward.
According to Boyle’s Law, under conditions of constant temperature, there is an inverse relationship between pressure and volume. This means that if pressure decreases gas volume increases. As such, by creating a negative pressure within the chest there is an increase in gas volume. Inspiration, where gas enters the lungs, is an active process during rest and exercise. At rest, the main muscle groups involved are the diaphragm and the intercostal muscles. During exercise there is further recruitment of accessory muscles to augment respiratory function. These include the sternocleidomastoid and the scalene muscles predominantly. Other muscle groups that have been observed to be recruited during exercise include serratus anterior, pectoralis major and pectoralis minor, trapezius, latissimus dorsi, erector spinae among others.
Expiration is predominantly a passive process during rest; the diaphragm relaxes and the lungs return to a state known as the functional residual capacity (FRC) or end-expiratory lung volume (EELV). This is the state whereby the opposing elastic recoil forces of the lungs and chest wall are in equilibrium. During exercise expiration becomes a more active process, with abdominal and intercostal muscles playing a greater role.
The lungs are attached to the chest wall via the pleurae. The visceral pleurae cover each lung and the parietal pleurae attach to the chest wall. Between each pleurae is a pleural cavity which contains a thin film of serous fluid. When air enters this space the lung can partially or fully collapse and the remaining air space is termed a pneumothorax.
How is breathing controlled?
Under resting conditions, small changes in ventilatory activity is controlled by the respiratory centre within the brainstem. These structures are centred in the medulla oblongata and pons. The medulla consists of two groups of neurons known as the dorsal and ventral respiratory groups and one within the pons, the pontine respiratory group. The latter includes two areas known as the pneumotaxic centre and the apneustic centre. There are several neural inputs into the respiratory centres that react to basic concentrations of oxygen, carbon dioxide and pH, but there are other inputs such as a response to hormonal changes and the ability to consciously control ventilation via the cerebral cortex.
In terms of the control of ventilation, under normal conditions of exercise, the predominant driving factor underpinning ventilation is a direct response to an increase in circulating concentrations of carbon dioxide. A bi-product of aerobic metabolism is carbon dioxide, an increase of which is detected by the respiratory centres and there is a concomitant increase in ventilation.
As exercise intensity increases aerobic metabolism must be supplemented by anaerobic metabolism. This anaerobic metabolism produces lactic acid which must be buffered by the bicarbonate system. This buffering process produces additional carbon dioxide to that of aerobic metabolism and hence ventilation increases further. Although this has been the standard explanation for the additional carbon dioxide produced during exercise, there is some contention within the literature, a summary of which can be found in sources within the additional reading list (see below). As exercise intensity continues to increase there is a point whereby there is insufficient buffering of lactic acid and the concentration of hydrogen ions increases. At this point the increase in hydrogen ions is detected by the peripheral chemoreceptors in the carotid bodies and these now takes over control of ventilation.
Work of breathing and the sensation of breathlessness and dyspnoea
A sensation of breathlessness is common in both health and disease and can be caused by a number of factors.
Dyspnoea is defined as ‘a subjective experience of breathing discomfort that consists of qualitatively distinct sensations that vary in intensity’.
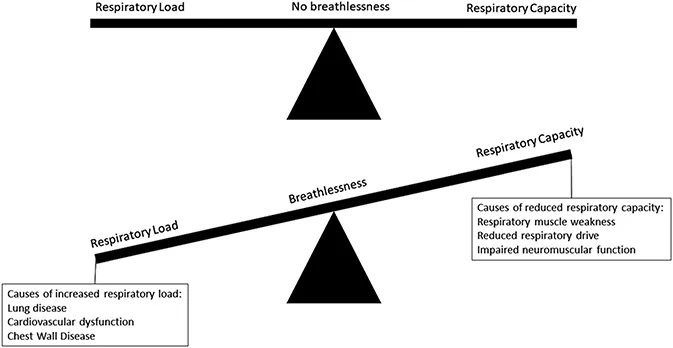
It is postulated that any factor that affects either the load on the respiratory muscles, their capacity or both will increase neural drive from the medullary respiratory centre to the respiratory muscles (Figure 1.1).
Increased neural respiratory drive is produced to ensure respiratory homeostasis.
When respiratory load and capacity is imbalanced it results in the sensation of breathlessness (Figure 1.1).
Figure 1.1 Influence of respiratory load and capacity on breathlessness.
How does airflow in the respiratory tract at rest and during exercise?
The airway tract includes the nasal cavity, larynx, large central airways (i.e. trachea and main bronchi) and smaller airways. During passive resting breathing most individuals will breathe through the nose and this pattern of ventilation is preferable; the lungs function best in warm and moist conditions and the nose, with its rich plexus of capillaries, acts to warm and humidify air from the atmosphere. The nose also acts as the first line of defence, filtering out particles and infective pathogens that have the ability to damage the lungs, via cilia and increased mucus secretion.
During exercise, as the demand to increase ventilation rises, individuals will begin (usually at approx. 35 L/min) to alter their respiratory pattern to utilise the combined oral and nasal route.
Given the resistance in the nasal cavity, it is not possible or feasible to generate sufficient airflow, via a predominant nasal breathing route, during moderate to strenuous exercise. It is therefore not logical to promote a nasal breathing pattern in athletes engaging in strenuous exercise. Moreover, there is no robust evidence that use of nasal strips or other devices to dilate the nares, is beneficial in enhancing nasal ventilation.
Any nasal obstruction arising from clinical conditions such as nasal polyps or rhinitis (see chapter 8), may force an affected individual to utilise an oral predominant breathing pattern at rest and this has deleterious implications for airway hydration, upper airway discomfort and risk of infection. As atmospheric air travels through the oro-nasal cavity there is exposure to lymphoid tissue in the form of adenoid, tubal, palatine and lingual tonsils that act as another line of defence, detecting pathogens and eliciting an immune response.
How does the larynx act as the bottleneck of the airway?
The laryngeal inlet represents a ‘bottleneck’ to airflow and is the last structure where there is common passage of both food and air; the lungs being protected from aspiration via the glottis. The larynx contains the vocal cords, which in conjunction with arytenoid cartilage, are used to produce sound for speech. During normal function these structures do not impact ventilation during exercise. However, in some individuals these structures may function abnormally to restrict the flow of air in and out of the lungs during strenuous exercise. Exercise-induced laryngeal obstruction (EILO) is now recognised to be highly prevalent in adolescent athletes with some studies indicating up to one in ten young athletes may have this condition, causing breathing difficulties during exercise (see Chapter 9).
What path does the air take to move from the trachea into the lungs?
Air enters the more distal airway tract via the trachea, which is a cartilage rich structure containing cilia and rich in seromucus glands, acting as another line of defence aiming to prevent pathogens and particles from entering the lungs. The trachea then divides into the two primary bronchi and this continued bifurcation continues all the way down to the alveolar ducts where the majority of gas exchange takes place. Weibel’s model of the airways classifies each bifurcation of the airways as one generation. There are approximately 23 generations of the airways with air travelling via bulk flow through the conducting airways down to approximately generation 16–17. From here air travels to the alveoli via diffusion and from this point onwards gas exchange begins to take place with the major gas exchange occurring within the alveolar ducts and individual alveoli.
With increasing airway generation there is a reduction in cartilage tissue. Airway tone is thus maintained via an increase in smooth muscle, which under normal conditions contracts and relaxes appropriately to external factors. In the presence of heightened bronchial hyper-responsiveness, there is an exaggerated smooth muscle response with increased smooth muscle contraction causing a reduction in airway patency that then impacts on exercise ability.
Increased exercise intensity, with a potential concomitant reduction in humidification and warming of air entering the lungs as explained above, can increase the osmolality of the airways eliciting a cascade response leading to airway constriction via exaggerated smooth muscle contracti...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Table of Contents
List of figures
List of tables
List of contributors
Foreword
Prologue: Why bother monitoring and optimising breathing issues in athletic individuals?
1. The respiratory system and exercise
2. Respiratory limitations to exercise
3. The environment and its impact on respiratory health
4. Epidemiology and pathophysiology of exercise-induced bronchoconstriction in athletes
5. Diagnosis of exercise-induced bronchoconstriction
6. Pharmacological treatment of asthma-related issues in athletes
7. Non-pharmacological management of asthma-related issues in athletes
8. Nasal problems in the athlete
9. Exercise-induced laryngeal obstruction
10. Dealing with respiratory infection in athletes
11. Breathing pattern disorders in athletes
12. Role of respiratory muscle training to treat exercise respiratory symptoms
13. Epilogue: Bringing it all together to optimise athlete respiratory care
Acknowledgements
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Complete Guide to Respiratory Care in Athletes by John Dickinson, James Hull, John W. Dickinson,James H. Hull,John Dickinson,James Hull, John W. Dickinson, James H. Hull in PDF and/or ePUB format, as well as other popular books in Medicina & Enfermedades y alergias. We have over 1.5 million books available in our catalogue for you to explore.