I recommend this scholarly and readable book to all concerned with the field of stress and trauma. Students and clinicians will find it equally beneficial.
Mardi J. Horowitz, M.D. Professor of Psychiatry, University of California, San Francisco and author of Stress Response Syndromes and Treatment of Stress Response Syndromes
This is a remarkably good book. One seldom sees such exquisite balance of scholarship, practical relevance and compassion for both client and counsellor. I recommend it most highly.
Michael J. Mahoney, author of Constructive Psychotherapy and Human Change Processes
Understanding Trauma and Emotion is an essential reference for all clinicians working in the area of trauma . . . and provides a comprehensive and very accessible account of the emotion-focused model of psychological trauma.
Michelle A. Webster, PhD, Institute for Emotionally Focused Therapy, Sydney
How do we help the traumatised?
How can we better understand someone who has faced death, violence or imprisonment?
Traumatic experiences can leave an indelible impression on those involved, one which the person may suppress or re-live with destructive and troubling consequences. For many traumatised individuals the essence of their trauma is deeply emotional: terror, anger, anxiety.
Colin Wastell interprets the modern understanding of the traumatic process and presents his own model based on extensive research. He examines the role of emotion in human function and in particular its role in the experience of trauma and effective trauma treatment.
Wastell's approach is grounded in practical treatment and the way emotion-focused therapy can be used to benefit the therapist and client. Using extensive case studies and making clear links between theory and practice, Wastell presents an innovative practice manual for the counsellor and psychologist interested both in trauma treatment and human emotion. These principles for understanding trauma will also assist health professionals, including nurses, doctors, ambulance officers, social workers, religious leaders, emergency services workers and police officers, to help their clients.
This book is also supported by a website, containing a full report of the author's research at: www.allenandunwin.com/trauma.asp
eBook - ePub
Understanding Trauma and Emotion
Dealing with trauma using an emotion-focused approach
- 224 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
Education General1
TRAUMA
This chapter begins with an outline of the impetus for the modern study of trauma. It then goes on to examine the contribution of two famous French traumatologists, Charcot and Janet. Of course, no discussion of the origin of modern trauma study would be adequate without a review of the work of Freud. The great conflicts of the twentieth century produced a tremendous amount of suffering and trauma, and a consequent focus on treatment and theory. The work of Abram Kardiner is described and the central importance of his work commented upon. The societal revolutions of the latter half of the twentieth century led in the West to the examination of sexual and domestic violence and trauma. We focus on these discussions by examining both the diagnosis of PTSD and a proposal for an integrated model of trauma.
A brief introduction to the study of trauma
The study of trauma (a term used here and throughout this book to refer to psychological trauma) is relatively new, though the phenomena has existed since humans began to be aware of their existence. The study is also the product of a complex interplay between human needs and social expectations. The formal study of trauma has a history of only about 150 years. It emerged due to changes in social structures, medical advances and philosophical outlooks. The material that follows is designed to provide an overview of the contexts of the models of trauma and their consequences for the way survivors of trauma have been viewed and treated.
Financial compensation and the modern study of psychological trauma
The Industrial Revolution in Europe and North America was a period of great change, particularly in terms of transport. The rise of railways across the globe meant that, for the first time, great numbers of people could travel at unprecedented speeds. Along with this great mobility came the potential for terrible accidents. At this time, the West was experiencing a period of great wealth creation, and also the expansion of middle-class political power. Railway accidents thus led to legal action for compensation, a problem which became the focus of political concern. The British government brought in the Campbell Act of 1846, which was revised in 1864. This act authorised compensation payments to victims of accidents. The 1864 amendment authorised payment to survivors of railway accidents. There were similar Acts in France which authorised monetary gain as a result of the reporting of injuries from accidents. In the case of trauma unaccompanied by physical injury, the suspicion emerged that the claimant may not actually be affected, but rather attempting to gain compensation by fraud. Erichsen (1883) contemptuously labelled the condition ‘railway spine’. The rise of interest in this condition was the beginning of the funded study of trauma. It is interesting, in this regard, that renowned French psychologist Charcot was requested to look into the phenomena of ‘railway spine’ by an insurance company. As the symptoms of ‘railway spine’ were studied, it became clear to some that they were very similar to ‘hysteria’—which was believed only to occur in women. The association of trauma with monetary compensation and with a ‘disorder’ associated with women resulted in a large degree of suspicion being directed towards those who claimed to be afflicted with trauma. Indeed, it is consistent with later literature that, from the point of view of the legal profession, if a person displayed the symptoms associated with trauma, they were either malingering or constitutionally weak (remember that women at this time were considered the weaker sex). This was not the whole picture, however. Some researchers and clinicians who were studying those afflicted with trauma were more focused on the condition than its financial or political contexts. For example, Briquet (1859, quoted in Mai and Merskey 1980) had examined women suffering from hysteria and noted that there was a high incidence of childhood trauma involved.
The Third Republic of France and French traumatologists
The political situation in France in the latter half of the nineteenth century led the period to be termed the ‘Third Republic’. One aspect of this political situation was that the secular governments of the time were staunchly anti-clerical. One of the deep desires of the Third Republic was to extol the virtues of science in opposition to superstition—by which was largely meant religion. The Roman Catholic Church had great influence in France, particularly among French women. If the Third Republic was to wrest more and more power away from the church, then it had to show that science was able to describe and understand people—especially women. The nature of women in this society was taken to be an important question for study. The focus of such study was not a form of early enlightenment about women’s rights; rather, it was part of the struggle between state and church. It is in this context that two great traumatologists made their very important contributions to the study of trauma: Jean Charcot and Pierre Janet.
Charcot
In addition to his early work on trauma, Charcot’s general psychological work was very significant for a number of reasons which are beyond the scope of this book. Using hypnotic suggestion, he studied women with a range of disorders. He connected suggestibility to hysteria, and was able to implant physical behaviours into patients under hypnotic trances. This had the result that the physical features of hysteria could be simulated in hypnosis. The famous demonstrations he conducted became legendary throughout Europe. Figure 1.1 shows the famous painting by Brouillet depicting one of these demonstrations. The painting also clearly illustrates the French attitude to the study of women with hysteria. The room is full of men in the pose of experts, scientifically studying the swooning woman. However, Charcot’s work was significant in that he asserted that symptoms of ‘real’, as opposed to induced, hysterics were the result of the women’s traumatic experiences. His reputation and standing meant that the scientific community was forced to consider the assertion that psychological events could produce physical symptoms that were not under the volitional control of the individual. However, by his demonstration that symptoms could also be implanted into subjects who were not traumatised, Charcot raised the possibility that some sufferers were in fact malingering or simulating their symptoms. The concept of simulation was taken up by his followers, with discussion concerning the exertion of the will. This led to a view that becoming traumatised was a matter of the sufferer having a weak will. In essence, the survivor of trauma became responsible for their own symptoms, since they were perceived as weak willed.

Figure 1.1 Brouillet’s painting of a Charcot demonstration of hysteria and accompanying caption (Ellenberger 1970, p. 330)
‘A Clinical lecture at the Salpêtrière.’ Brouillet’s painting shows Charcot at the height of his fame, demonstrating a case of ‘grand hystérie’ to an elite audience of physicians and writers; behind him is his favourite disciple, Babinski. The painter has involuntarily shown Charcot’s fatal error: his verbal explanations and the picture on the wall suggest to the patient the crisis which she is beginning to enact; two nurses are ready to sustain her when she falls on the stretcher, where she will display her full-fledged crisis.
Janet
The work of Janet in the period 1890–1910 was very significant for the development of the psychological view of trauma. His work was not studied extensively until the last decade and a half (van der Kolk and van der Hart 1989). It was Janet who noted the impact of ‘vehement emotions’ in the experience of trauma. By ‘vehement emotions’, he meant terror and fear. This insight is important, since it points to the critical role of emotion processes in trauma. Janet suggested that the result of these emotional reactions was to give rise to a kind of split existence. He maintained that the painful memories became locked into a kind of unrecited memory which simply replayed and replayed but was never integrated. He asserted that, because the memories were so painful, they could not be recited as part of one’s personal narrative. He further claimed that the agitation produced was of no adaptive value, and thus became an insurmountable obstacle in the life of the traumatised person. It was Janet who asserted that dissociation was the core of the pathological process involved in trauma. The work done on the dissociative process led him to develop the concept of simultaneous consciousness—that is, the idea that consciousness is not one-dimensional. The clear implication of this is that there are layers to the processing of human experience, and that what is seen in sufferers of traumatic neurosis is the result of an unsuccessful attempt to process the vehement emotions. Janet, like Charcot, also asserted that hysteria was the product of real trauma.
Sigmund Freud and trauma
No introduction to the study of trauma could be undertaken without an examination of the work of Sigmund Freud. Freud studied under Charcot and knew of the work of Janet, although Freud always denied that any of his theory was taken from Janet. There are similarities but these may simply be the product of a common mentor—Charcot. Freud discussed (Jones 1953, p. 226) the case of hysteria, of Anna O, with Breuer in the early 1880s before he went to see Charcot. Freud did not treat this case, but it shows that he was aware of the condition before actually seeing Charcot. Freud was very much in awe of Charcot. Freud refers to Charcot as the ‘greatest of physicians’ (Jones 1953, p. 185). He spent about five months with Charcot—although he notes that he was initially one among many. Freud responded to a request by Charcot for someone to translate his works into German, and produced a translation of some of Charcot’s work as early as 1886, which allowed Freud into Charcot’s inner circle.
Charcot’s assertion that symptoms of ‘real’ hysterics resulted from traumatic experiences, and that hysteria occurred in men as well as women, was a very confronting concept at the time. Freud’s theory that hysterical paralysis was the result of ‘popular conceptions’ rather than of anatomical facts was also revolutionary. Freud demonstrated that certain physical symptoms of hysterics were not consistent with the anatomical structures of the human nervous system.
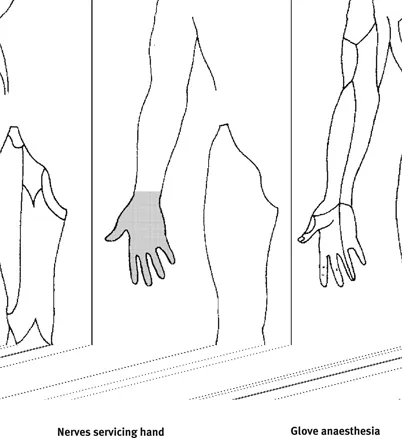
Figure 1.2 Glove anaesthesia (Erdelyi 1985, p. 3)
The famous case of glove anaesthesia is a very good example of this. A woman reported having no feeling in her hand. The pattern of this anaesthesia was consistent with the area covered by a women’s glove (see Figure 1.2). When Freud pricked the hand with a pin, the woman showed no sign of pain in the afflicted area. However, the region suffering this condition was not consistent with the pattern of nerves servicing the human hand. What had produced this induced state of anaesthesia? Was the human mind capable of producing physical effects that were able to control the conscious registration of nerve impulses? Freud was very keen to spread the views of Charcot once he returned to Vienna, and presented a paper on male hysteria not long after returning from Paris in 1896. The discussion that followed within the profession was an example of professional resistance to the concept of trauma. Many rejected the connection between trauma and hysteria, and Freud was confronted with the establishment’s views on male hysteria and trauma.
Between 1892 and 1896, Freud published and lectured on his work with women who suffered from hysteria and other maladies. Freud, like Janet, viewed dissociation as the core of the problem of hysteria. As a result of several famous cases involving Breuer and also Freud, there arose a theory of hysteria that was a shock to Freud himself. Freud and Breuer asserted that the women were suffering from hysteria as a result of their actual experiences of sexualised contact as children. From his work with patients, Freud determined that the process of traumatisation had two main aspects: first, the events were so terrible that they left an emotion-charged residue in the psyche; and second, this produced altered states of consciousness in which the trauma was encased. The basic process of the development of neurotic symptoms is shown in Figure 1.3.
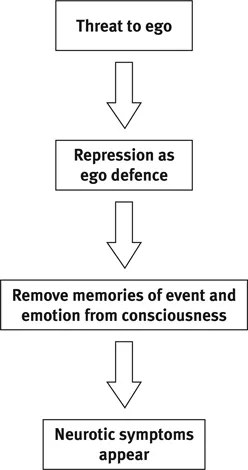
Figure 1.3 Freud’s model of the development of neurotic symptoms
This is the process for all ‘traumatic’ events. The process involves the generation of very powerful emotions that threaten to overwhelm the ego’s ability to function. This is the context of Freud’s often-quoted statement that people with hysteria ‘suffer from reminiscences’ (Breuer and Freud 1893–95). Memories are charged with strong emotion, or are highly stylised and emotionless. Freud cited clinical examples of ‘intact’ memories of traumatic events and noted the strong emotions that were expressed by patients. The alarming implication of this finding for Freud was that the traumatising events were being perpetrated in the home by family members. Here was the first instance of the study of trauma pointing to some very disturbing aspects of Western family life, structure and character. Freud published his findings concerning the link between hysteria and sexual abuse in 1896. This model is referred to as the seduction theory.
Society’s reaction to the seduction hypothesis and its consequences
Society’s reaction to Freud’s seduction theory was one of mixed fascination and outrage. Typical of the reaction was that of C.H. Hughes, in the journal Alienist and Neurologist (1896), who described the assertions in Freud’s seduction theory as ‘grave’ and went on ‘to condemn the absurdity of such...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Dedication Page
- Acknowledgments
- Contents
- Figures and tables
- Introduction
- 1 Trauma
- 2 Emotion processes and trauma
- 3 Emotion and trauma treatment
- 4 Treatment of circumscribed trauma
- 5 Treatment of complex traumatisation
- 6 The trauma therapist and their emotions
- 7 Traumatic dissociation
- Appendix A DSM III-R Criteria
- Appendix B DSM IV TRCriteria
- Appendix C The ICD-10 Classification of Mental and Behavioural Disorders
- Glossary
- References
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Understanding Trauma and Emotion by Colin Wastell in PDF and/or ePUB format. We have over 1.5 million books available in our catalogue for you to explore.