This textbook provides a brief review of pediatric medicine practice. This book covers the diseases and disorders commonly seen in routine practice. The chapters cover pediatric disorders such as obesity, gastroesophageal reflux, asthma, bronchiolitis, pneumonia, allergy, sinusitis, diabetes, thyroid disorder, epistaxis, otitis media, hearing loss, laryngomalacia, obstructive sleep apnea, central sleep apnea, laryngomalacia, stridor, tonsillitis, haemophilia, autism, and anxiety.
Key features of this textbook include:
- Reader friendly format which explains etiology, pathophysiology, and disease management
- 21 chapters covering common pediatric disorders encountered by medical professionals
- Contributions by several experts in pediatric subspecialties
This textbook is a suitable reference for medical students, interns, residents, and specialists including pediatricians, family medicine practitioners, otolaryngologists as well as subspecialists such as pediatric cardiologists, pulmonologists, endocrinologists, otolaryngologists and allergists.
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Synopsis of General Pediatric Practice
About this book
Information
Topic
MedicineSubtopic
Pediatric MedicineSynopsis of Management of Diabetes Mellitus Types 1 and 2
Eric Velazquez, Bethany A. Auble*
Medical College of Wisconsin, Children’s Hospital of Wisconsin, Milwaukee, Wisconsin, USA
Abstract
Diabetes involves pancreatic dysfunction due to autoimmune destruction of the beta cells and insulin deficiency. The prevalence and incidence of Type 1 and Type 2 are increasing in the general population. Type 1 Diabetes often begins in childhood and requires lifelong insulin replacement therapy and monitoring of blood glucose levels. Long and short-acting insulin allows for adjustment of therapies around patients’ lives, but close medical observation and a good patient-provider relationship is necessary for optimal management. Type 2 Diabetes is characterized by severe insulin resistance and partial deficiency that has become more prevalent in pediatric patients, often occurring around puberty. Therapy involves lifestyle changes to promote active weight loss, healthy eating habits, and exercise. Few pharmacological therapies are approved, but many are being studied for pediatric use.
Keywords: Artificial Pancreas, Bariatric Surgery, Closed Loop Control, Continuous Glucose Monitoring, Continuous Subcutaneous Insulin Injection, Glucagon, Insulin, Lifestyle Changes, Metformin, Multiple Daily Insulin Injections, Type 1 Diabetes, Type 2 Diabetes.
* Corresponding author Bethany A. Auble: Medical College of Wisconsin, Children’s Hospital of Wisconsin, Milwaukee, Wisconsin, USA; Tel: 414-337-8717; Fax: 414-266-6749; Email: [email protected]
INTRODUCTION
Diabetes Mellitus is a life-altering diagnosis, requiring adjustment of a patient’s life and schedule. In pediatric patients, it also changes the entire family’s focus. Loss of insulin-secreting beta cells results in loss of glycemic control with subsequent hyperglycemia in Type 1 diabetes. Insulin replacement therapy remains the mainstay of current therapy. Advances in insulin pumps, continuous glucose monitors, and closed loop control systems have resulted in long-term improved glycemic control. New advancements in pancreatic transplant, stem cell therapy, biomarker screenings, and prevention strategies are being published yearly. Type 2 Diabetes requires an alternative approach to management with a
strong emphasis placed on diet, exercise, and lifestyle modifications. The medical therapies for the treatment of Type 2 Diabetes are a growing field of research, but pharmacotherapy must be combined with lifestyle changes if lasting health improvements are to be achieved.
Epidemiology
In the United States, the prevalence of Type 1 Diabetes is estimated for 0.25% of the population [1]. From 2001–2009, prevalence of Type 1 diabetes increased by nearly 20%, with projections suggesting that from 2010 to 2050, the number of youth with Type 1 diabetes may triple. In this same time period, the prevalence of Type 2 diabetes increased by nearly 30% and accounts for 45% of newly diagnosed cases of diabetes in the pediatric population. Projections suggest that from 2010 to 2050, a nearly 4-fold increase might occur of patients with Type 2 diabetes. While still relatively uncommon, the rates of new cases of type 2 diabetes were greater among peripubertal individuals aged 10–19 years than in younger children, with higher rates among U.S. minority populations than in non-Hispanic whites.
Physiology
The pancreas is both an exocrine gland and an endocrine gland. Endocrine cells are located within scattered Islets of Langerhans and divided into three categories: alpha-cells (produce glucagon), beta-cells (produce insulin and amylin) and delta-cells (produce somatostatin). Insulin stimulates cells to uptake free glucose, glycogenesis in the liver, and uptake amino acids, proteins and fat from the bloodstream. Humans are born with a varying amount of beta-cells, and even within these cells, there is variation to susceptibility to auto-immune attack [2]. In Type 1 Diabetes, autoimmune destruction of beta-cells produces gradual dysregulation of glucose and its symptoms develop after >80-90% of cells are lost. Type 2 Diabetes is caused by the relative deficiency of insulin due to severe peripheral tissue resistance.
Glucagon works primarily in the liver to convert glycogen into glucose to raise blood glucose. Its function becomes dysregulated in type 2 diabetes, leading to postprandial hypersecretion, worsening overall hyperglycemia. Amylin is a neuroendocrine peptide hormone that is co-secreted with insulin, uses the same processing enzymes, and works to suppress release of glucagon, slows digestion and slows rate of insulin entering the bloodstream. The benefit of delayed gastric emptying is creating a slower rise, and overall lower peak level of blood glucose [3]. Somatostatin is a peptide hormone that has many GI effects but is active in slowing gastric emptying, suppressing insulin and glucagon release, and suppressing exocrine pancreatic secretions. Incretins are small hormones released by intestinal mucosa that stimulate insulin release, delay gastric emptying and inhibit glucagon release. While native molecules have short half-lives, synthetic versions last much longer and are being looked at as therapeutic alternatives.
TYPE 1 DIABETES MELLITUS
The “event” of stage II most likely is not a single event but some combination of environmental and genetic triggers. The time period of stage III-IV is highly variable, the reasons for why are being closely studied [2]. Patients most often present with classic symptoms of onset: polyuria, polydipsia, hyperglycemia and ketonuria during Stage V (some present in full diabetic ketoacidosis). The “honeymoon period” between Stage V and VI is called such as very low supplemental insulin is required to maintain normoglycemia (Fig. 1).
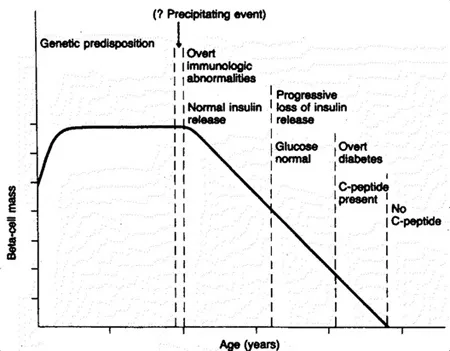
The Eisenbarth model for the development of Type 1 Diabetes is divided into six stages: 1. Genetic Predisposition, 2. Triggering “Event,” 3. Activation of Autoimmune Response, 4. Immunologic Response with progressive loss of insulin secretion with maintenance of normal blood sugar level, 5. Symptoms develop, but residual insulin secretion is maintained, 6. Loss of residual insulin secretion to a point of glucose dysregulation [4].
Hemoglobin A1c is the form of hemoglobin produced through nonenzymatic glycation within red blood cells. Production varies directly with plasma glucose levels. Monitoring concentration allows for idea of average glucose levels over the life span of the red blood cells (roughly 2-3 months). The ADA treatment guidelines recommend: HbA1C <7.5% in pediatrics, <7% in adults (lower for pregnant women), reduction in hypoglycemic events and prevention of long-term complications of poor glycemic control. Most adults are not meeting the ADA HbA1c goal, and patients 13-25 years old actually have the worst control based on HbA1c levels [5].
Multiple Daily Injection Insulin Regimens
Multiple Daily Injection (MDI) insulin regimen is the standard therapeutic approach of Type 1 Diabetes and involves calculating daily insulin requirement, basal insulin amount, carbohydrate coverage dosing, and meal-time sliding-scale bolus doses. Total daily insulin dose is highly variable, but is generally determined by the patient’s pubertal status (Table 1).
Table 1 Types of Insulin.
| Insulin Type | Examples | Onset of Action | Peak Effect | Duration of Action |
|---|---|---|---|---|
| Rapid-Acting | Insulin Lispro (Humalog), Insulin Aspart (NovoLog) Insulin Glulisine (Apidra) | 15-20 minutes | 30-90 minutes | 1-4 hours |
| Regular-Acting | Novolin R and Humulin R | 30-45 minutes | 2-3 hours | 5-8 hours |
| Intermediate-Acting | NPH (Humulin N, Novolin N) | 2-4 hours | 4-10 hours | 4-12 hours |
| Long-Acting | Insulin glargine (Lantus) Insulin detemir (Levemir) | 2-4 hours | No peak 8-10 hours | 20-24 hours Dose-related |
Use of a basal/bolus dosing regiment attempts to establish patterns that most closely approximate normal human physiologic release of insulin. Advantages for this style of dosing include: improved glycemic control, lower HbA1c, and may reduce hypoglycemic events overnight. Pre-meal injections allows for a more flexible meal-time schedule to accommodate lifestyle. The addition of carbohydrate coverage dosing allows for freedom of meal choice (e.g. high-carbohydrate meal will need more insulin; a low-carbohydrate meal will need less). Disadvantage of basal-bolus dosing of insulin is that multiple injections throughout the day are needed, and frequent glucose checks are also required. The number of fingerstick blood glucose checks and injections can be distressing to some patients. With the advent of insulin pump therapy, new basal-bolus approaches became possible (Table 2).
Table 2 Calculation of Insulin Requirements.
| Insulin | Dose Calculation | Calculation for 20 kg Child | Dose | |
|---|---|---|---|---|
| Total Daily Insulin Dose | 0.5 – 1.0 units/kg/day | 0.5 x 20 = 10 units/day | 10 Units | |
| Basal Dose | Glargine Detemir | 50% of total 50% of total divided into twice a day dosing | 50% x 10 = 5 units | 5 Units |
| Meal-time Glucose Correction | Lispro, Aspart Regular | 1800 / Daily Dose 1500/ Daily Dose | 1800 / 10 = 180 1500 / 10 = 150 | 1 unit for every 180 mg/dL > ideal glucose 1 U for every 150 mg/dL > ideal gluc... |
Table of contents
- Welcome
- Table of Contents
- Title Page
- BENTHAM SCIENCE PUBLISHERS LTD.
- PREFACE
- List of Contributors
- Update on the Management of Otitis Media
- Contemporary Management of Children with Hearing Loss
- Overview of Management of Recurrent Tonsillitis
- Therapies for Pediatric Chronic Rhinosinusitis
- Practical Management of Children with Stridor
- Update on the Management of Laryngomalacia
- Synopsis of Management of Diabetes Mellitus Types 1 and 2
- Pediatric Type 2 Diabetes Mellitus
- Practical Guide for Management of Children with Obesity
- Current Concepts in the Management of Hyperthyroidism
- Recent Advances in Pediatric Asthma
- Evaluation and Treatment of Bronchiolitis
- What is New with Management of Pediatric Central Sleep Apnea?
- Practical Considerations in the Treatment of Pediatric Obstructive Sleep Apnea
- State of the Art of the Diagnosis and Management of Gastroesophageal Reflux Disease
- Essentials of Sickle Cell Disease Management
- Management of Recurrent Epistaxis
- Update on Management of Allergic Rhinitis
- The Management of Pediatric Allergic Emergencies
- Autism Spectrum Disorder: What a Pediatrician Should Know
- Treating Anxiety in Children
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Synopsis of General Pediatric Practice by Seckin Ulualp in PDF and/or ePUB format, as well as other popular books in Medicine & Pediatric Medicine. We have over 1.5 million books available in our catalogue for you to explore.