![]()
The Discipline for Pastoral Care Giving
![]()
Introduction to the Discipline for Pastoral Care Giving
Arthur M. Lucas, MDiv, BCC
Summary. During the last eight years, the professional chaplains of Spiritual Care Services at Barnes-Jewish Hospital-Washington University Medical Center (BJC) have developed a discipline based, outcome-oriented model for chaplaincy. This article introduces the elements of
The Discipline, our development process, the effects on our chaplaincy attributable to its consistent use, and implications for the future. While many of our assumptions about chaplaincy have been challenged, our experience is that a disciplined, outcome-oriented model for chaplaincy has deepened our relationships with patients and significantly increased our integration into the care teams of the hospital. It has also challenged and enhanced our abilities to be emotionally present with patients while also giving attention to the process of the visits and chaplain interventions that contribute to patient healing and well-being.
[Article copies available for a fee from The Haworth Document Delivery Service: 1-800-342-9678. E-mail address: <[email protected]> Website: <http://www.HaworthPress.com> © 2000 by The Haworth Press, Inc. All rights reserved.] Keywords. Chaplain, pastoral care, measurement, outcomes, discipline
Introducing Barnes-Jewish Spiritual care as the Context for the Discipline
Since 1990, the chaplains at Barnes-Jewish Hospital (BJH) have sought to increase their integration into and accountability with the care teams. Carrying through these intentions led to far more than we anticipated.
We consciously maintained pastoral presence, relationship, and process at the core of our care. And we are now clear that our primary purpose is not simply to be in relationship to patients or aware of the process. Our purpose is to contribute to their healing and well-being, whatever that may mean for each of them. In the process of clarifying this for ourselves, we developed The Discipline and it greatly enhanced our integration and accountability in the clinical services for patients. And, more immediately, The Discipline enhanced our ability to engage the spirituality of the people in our care for their healing and well-being. We have also become more outcome-oriented, consciously attending to the effect of our care for our patients and families.
We entered this process with some value assertions and discovered others along the way. One assumption was that spiritual assessment was not about the size or good/bad of Spirit. Rather, we wanted to know how the spiritual functioned, what differences it made for and with the people in our care. We wanted to capture the difference it made in people’s lives. Another assertion we made at the beginning was that, in this spiritual assessment process, each of us was more a partner with the person and their spirituality than someone who needed to make it “right.” We were to perceive, respect, and engage this spirituality.
We immediately found that, when we emphasized these assertions in our pastoral care as well as our integration and accountability within the care teams, we also had to be more conscious of our pastoral care assessment, planning and reflection processes. We found that doing so led to:
- Evaluating and improving our care. When we were more conscious of our pastoral presence and process, knew how we knew who was before us, and what effect we were having, then we were more able to change the care we were giving. Deliberate evaluation either in the midst of the caring or upon reflection afterwards improved that care.
- Communicating our care more effectively with others. With the process more conscious, we made choices in the language through which we organized and communicated both the spirituality of the people in our care and our chaplaincy with them. We were then able to help other members of the care team to provide more whole, personally efficacious care as well.
- Seeing patterns in the struggling, coping, and healing of people. Health challenges, crisis, and treatment interventions seemed to be associated with discrete patterns. In a cumulative manner, we began to learn from patients/families about the unique spiritual dynamics associated with health care challenges as well as the spiritual care that seemed to hold the most promise for contributing to their healing and well-being.
From the beginning, several staff chaplains were involved in our development of The Discipline. They included Eric Affholter in HIV/AIDS Care, Robert Yim in Heart Services, Cheryl Palmer in Thoracic Services, and Julie Allen Berger in Oncology. Others joined us later, including Lawrence Olatunde in Trauma, Fred Smoot in Psychiatry, and Janet Crane in HIV/AIDS care. Each of us became more conscious of what we were learning from our clinical experience, more aware of what patients were teaching us cumulatively. Patterns emerged in the spiritual dynamics during life changing health care challenges as we looked at an individual case alongside the next, alongside the next, alongside the next, to the hundreds of clinically/ diagnostically similar cases.
Our cumulative learning was enhanced (or perhaps made possible) by assigning individual chaplains to discrete clinical areas. This allowed each chaplain to focus on the spirituality of patients in distinct clinical contexts and identify patterns of spiritual challenges. These clinically similar patients provided us focused, repetitive opportunities to learn how best to engage their spirituality for optimum outcomes.
Cultivating a deliberate, disciplined reflection process also helped us see patterns. Rather than seeing only the uniqueness of each patient story, we began to see commonalities. We found similar spiritual dynamics for patients who were clinically similar even when they might be religiously dissimilar.
We began to observe three primary spirituality patterns among patients. The first concerned how spirituality was operating. The second focused on the function of spirituality or what it was called on to do, and third, what effect spirituality seemed to have. These three helped us see the similarities of the dynamic and the functional levels involved. Based on these patterns, we were able to focus more clearly and quickly on the critical spiritual dynamics for patients who were dealing with specific clinical realities in specific contexts. Focusing with intentionality made it easier for us to meet, honor and engage spirituality for patient healing and well-being.
Seeing these patterns reminded us of creative tensions in which we were now more consciously living. This first tension was between the unique individual on the one hand and generalizable dynamics on the other. Our previous training had taught us to distrust the general/universal and always depend on the particular, the unique, the individual for pastoral understanding. When we also began to see the spiritual commonalities, we felt bound to accept what individual patients taught us for the benefit of others. We still could not settle comfortably into “knowing” how all heart or cancer or thoracic patients “were.” We still saw too much individuality, were surprised too many times, and still believed deeply in the richness of creation. Nor could we revert to self-induced ignorance about the experiences of patients so that we could overlook what they taught us. We were left with the creative tension between individuality and common patterns.
A second creative tension was between presence/process and doing/ outcomes. We had learned in seminary and/or CPE that doing “nothing” was a primary value of a pastoral care giver in health care. Phlebotomists, respiratory therapists, nurses, and doctors went into patient rooms with tools and technologies to do things. As pastors, we entered with our personal, emotional availability and tried to be “present” with patients. In that way, we assured our attentiveness to patient feelings, faith, personhood, and agenda as we tried to be faithful vessels of the Spirit, journeying with them. As taught, we embraced this lack of control and believed it provided a healing counterpoint to technologists. Unfortunately, the implication of not being in control, especially on the spiritual level, involved disowning intentionality. We avoided intentionality about what was likely to be good for patients because it would be controlling. Intentionality meant we were imposing values and agenda, putting predetermined criteria above the person just as we believed the science/technology-based caregivers were doing.
In our explorations, we found being present with patients can include informed intentionality. We found that the spiritual process of the pastoral visit can be enriched by attention to what we can contribute. If we intended good to come from our care, what good? As soon as we could identify the intended good, we were dealing with outcomes. More precisely, we were dealing with “contributing outcomes” because our contributions were among those made by all the other care givers.
Another way to understand “contributing outcome” is to think of the benefits contributed by every member of the health care team. Each contributes in their own way to a desired outcome that hopefully furthers patient well-being. The final outcome, of course, takes a variety of forms. It may mean a peaceful death, a meaningful life that integrates a chronic illness, or a return to a lifestyle that preceded the illness. For instance:
- A well-done coronary artery bypass graft surgery has the promise of the “contributing outcome” of returning blood flow to the heart. The surgery is an activity (or intervention); the hoped for good (contributing outcome) is the return of blood flow to the heart which should contribute to an intended thriving recovery from heart disease.
- A well-done radiation treatment series promises the “contributing outcome” of reducing the tumor size for a cancer patient. The radiation treatments are activities (or interventions), the hoped for good (contributing outcome) is the reduction of the tumor which should contribute to an intended remission or reduction of the cancer in the patient’s life.
As we built The Discipline, we experienced the profound challenge of giving attention at the same time to both contributing outcomes and the more traditional process orientation. We were stretched both conceptually and personally by our attempts to hold these two in tension.
Notice that the idea of control was excluded from our resolution of this core tension. We concluded that it is a seductive fantasy in any framework. The challenge is to look elsewhere for substance and accountability.
Resolving either of these two tensions described above by going to one of the poles now seemed insufficient. The reality of the patient’s life changing situation outstripped the coziness of either pole. The complexity of what it took to be a caring presence in those realities denied the simple comforts of certainty offered by either pole. We learned we could live and thrive without the polar comforts once we realized that none of this was really about us, the care givers. It was about those in our care and their healing. That made the challenges and uncertainties of living within these tensions worthwhile and more appropriate to the real life complexities confronting our patients.
Introducing the Discipline for Pastoral care Giving
As the staff chaplains began to observe patterns among the patients, I, as department director, began to observe the patterns within the chaplaincy. The two processes began to feed each other. Even given the uniquenesses of staff chaplains and clinical contexts, a pattern ran through their most compassionate, faithful and effective care. The pattern in their chaplaincy became the basis for The Discipline for Pastoral Care Giving.
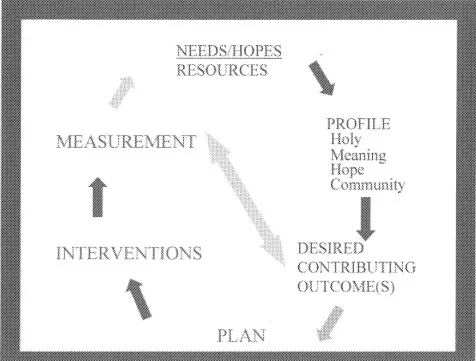
I will introduce each element of The Discipline separately and in more depth, but first, step back to see a sketch of the whole process as displayed in Figure 1.
- The Discipline always, always starts with the Needs, Hopes, and Resources of those to whom we are providing care, whether they are patients, residents, family, staff, ourselves, our students, or entire nursing units and departments. While the focus of our care always varies, our engagement always starts with attending to their Spiritual Needs/Hopes/Resources.
- Attending to Needs, Hopes and Resources provides the living material for developing a structurally consistent, Profile of the people to whom we are providing care. By wondering how their faith functions in life and what differences their spirituality can make in their life changing situations, we sketch out their sense of the Holy, Meaning, Hope and Community.
- Once we are into the processes of getting to know people and organizing what we are learning, we focus on getting some idea of the Desired Contributing Outcome (s) for this patient/family. What can our ministry contribute to this person’s healing and well-being? What difference do we hope to make?
- Once we have identified contributions we hope to make to the patient’s healing, we develop and share a Plan for how we together can move toward those contributing outcomes and what our distinct pastoral role is in the plan.
- With a plan in mind we can provide specific Interventions based on that plan, specifically those unique to spiritual care.
- Then it is appropriate to Measure the actual outcomes of our care against the desired contributing outcomes we had in mind.
- And then, perhaps we need to cycle right back around to a new assessment of needs, hopes, and resources.
Figure 1
© Chaplain Arthur M. Lucas. Reprinted with permission.
As you read more about each aspect of The Discipline, note that however specific or focused the components, it remains largely content free. It is a model awaiting each application. While it forms a map, a structure outlining the flow of the care giving, it is dependent on the patient/family for substance and applicability. We are partially alerted to that substance by what previous patients have graciously taught us. For the care of a person facing a health care crisis, the structure of The Discipline and the most carefully identified patterns are utterly dependent on the individual before us for substance and meaning. The Discipline only helps provide focus, communication, reflection, and accountability. Doing so then aids effectiveness.
Needs, Hopes, and Resources
The Discipline always starts with the Needs, Hopes and Resources of whomever is the focus of your care. The traditional approach starts with patient needs. The caregiver finds out th...