![]()
Chapter 3
Health status and key interventions
Understanding key technical interventions for improving maternal health and child health and recognizing how these interventions relate to one another is a prerequisite for making strategic choices about health sector policy and programs. This chapter lays out disease-specific causes of mortality and morbidity, presents estimates (where possible) of the prevalence or the burden of disease associated with those conditions, and describes the primary interventions to address each.
Connecting maternal health and child health
Although child health and maternal health interventions are examined in separate subsections, as lived experience and as a matter of biology they are sometimes— but not always—closely related. The chapter uses a lifecycle approach and the concept of sexual and reproductive health and rights to explicate these relationships. The lifecycle framework is useful for understanding connections over time, as health events at one stage influence health at a later stage across the life span and influence the next generation through the life cycle. The sexual and reproductive health and rights framework is useful because it grounds us in the all-important social, cultural, and political contexts of health. In particular, it reminds us that none of the health interventions considered here “falls like manna from heaven” (Wagstaff and Claeson 2004). Not only must the health system be organized to ensure its availability, but—barring coercion—each woman must make an active decision to use it for herself or her children. That decision will be made from within the tighter or looser web of constraints that bind her specific lived reality (Petchesky and Judd 1998; Shepard 2000).
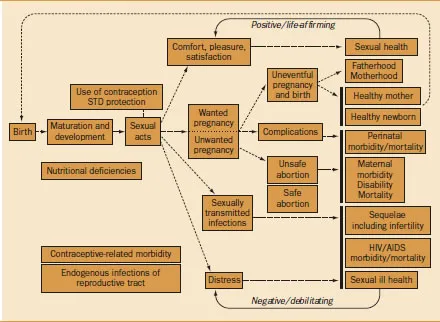
A sequence of interactions and events frames the experience of sexual and reproductive health over the lifespan (figure 3.1).1 The conceptual map shown in figure 3.1 is two-dimensional, but as its authors note, the map could also be imagined in layers (Cottingham and Myntti 2002). The base layer is the framework depicted in figure 3.1, including processes (such as maturation), events (such as pregnancy), and outcomes (such as pleasure or distress, health or disease)—simply moving through the stages of life. Superimposed on this base could be a layer of social and institutional arrangements that influence the way in which the different stages are experienced. These social and institutional arrangements include intimate and family relationships; community institutions, such as schools, religious institutions, the media, and the market; preventive and curative healthcare services; and governmental institutions, including the laws and policies they are responsible for implementing.
Figure 3.1 Conceptual map
of sexual and
reproductive health | |
Source:Adapted from Cottingham and Myntti 2002. Reprinted with permission from MIT Press.
| Women's agency is positively correlated with women's health and children's health | Such social and institutional arrangements influence the way events depicted in the map are experienced, because these arrangements function as the repositories of power and resources that individuals draw on to protect their health and prevent or treat disease (Link and Phelan 1995). These resources include not simply economic resources but also such nonmonetary assets as social networks, prestige, education, information, and legal claims. For example, a woman who, because of access to resources such as education, legal claims to gender equality, and strong social networks, has been able to obtain formal employment and achieve financial independence is likely to have greater power to negotiate the conditions of intimate relationships, including use of contraception, and to have the resources to obtain the contraceptive that best meets her needs. The constellation of power and resources—the assets— that this woman accesses through multiple social and institutional arrangements thus influences her experience of the box in figure 3.1 labeled “use of contraception/STD protection” and the subsequent sexual and reproductive health stages in the map (sexual acts, wanted/unwanted pregnancy, comfort/ pleasure/satisfaction, and so on). |
| These assets are not evenly distributed in any society. Gender, class, race, and ethnicity are intersecting social hierarchies that often act as a grid of inequality through which an individual's experience of the social and institutional arrangements is filtered. Imagined this way, the map helps conceptualize the mechanisms by which inequality in access to power and resources ultimately affects health. |
The map also clarifies the critical relationship between sexuality and reproduction, making the important point that many aspects of sexuality are separate from reproduction and have consequences—both positive and negative— for physical and mental health independent of pregnancy and childbearing (Miller 2000). This point becomes critical for developing effective interventions, including strategies for preventing the transmission of HIV. It is also a crucial point in understanding some of the controversy that has sometimes blocked health interventions.
Sexuality and reproduction—both separately and together—are at the core of the intimate, economic, and institutional relationships that characterize both women's oppression and their potential for determining the course of their own lives, that is, for their agency. As the UN Millennium Project Task Force on Education and Gender Equality elaborates in its report, agency is a basic component of gender equality, itself a Goal. As assessed through various indicators of women's status and empowerment (such as control over income and education), agency is in turn positively correlated with aspects of women's health (Lule and others 2003; Barnett and Stein 1998) and children's health (Hobcraft 1993; Wagstaff and Claeson 2004). Thus agency becomes a core principle of sexual and reproductive health, best expressed in the legal concept of sexual and reproductive rights (see box 2.2).
Figure 3.1 refers to both men and women and to both fatherhood and motherhood. The health literature rarely connects the health of children to the health or even the actions of their fathers, apart from genetics.2 In societies gripped by epidemics of sexually transmitted infections, including HIV/AIDS, this is a dangerous omission. Although newborns contract HIV from their mothers, virtually all HIV-positive pregnant women contracted HIV from the men with whom they have sexual relationships. The sexual and reproductive health of men, and men's actions, can therefore have a significant effect on the health of both women and their children.
Child health
| In parts of the world, progress in reducing child mortality has stalled | Important gains were made in child survival during the second half of the twentieth century (Freedman and others 2003). Globally, the under-five mortality rate (the number of deaths per 1, 000 live births per year) declined from 159.3 in 1955–59 to 70.4 in 1995–99 (Ahmad, Lopez, and Inoue 2000). The decline was most rapid during the 1970s and 1980s. Although the rate of decline slowed during the 1990s, child mortality still fell about 15 percent during that decade. This was an impressive achievement given the events that affected international public health development programs toward the end of the twentieth century— economic stagnation, increasing political instability and conflict, growing resistance to antimalarial drugs, and the relentless spread of the HIV/AIDS pandemic, to name a few. Overall the number of children under the age of five who die in the world each year fell from about 13 million in 1980 to an estimated 10.8 million by the end of the century (Black, Morris, and Bryce 2003). |
Despite these gains, more recent trends suggest that there is serious reason to be concerned. The rate of mortality decline seems to have slowed considerably. Part of the decline reflects the fact that very low rates have already been achieved in Europe, the Americas, the Western Pacific, and the Eastern Mediterranean (to use the geographical divisions of the WHO). But the decline also reflects failure to make progress in Sub-Saharan Africa and Southeast Asia. In fact, in a few countries, notably those in southern Africa, where AIDS is taking its greatest toll, child mortality rates have stagnated and even begun to increase.
In 2003 a major review of child mortality was undertaken that addressed disease-specific causes of death and the potential of available public health interventions to prevent them. From a series of articles published in The Lancet and in a number of meetings held to discuss the findings and recommendations, six themes emerged:
- A small number of diseases and underlying biological factors are responsible for the large majority of childhood deaths.
- The Goal for reducing child mortality cannot be met without a major effort to reduce newborn deaths—those that occur during the first four weeks of life.
- Existing interventions, if implemented through efficient and effective strategies (in a way that reaches those who need to be reached), could prevent a substantial proportion of existing mortality.
- Child mortality is distributed in an extremely uneven manner. Not only between regions and countries but also within countries, socioeconomic inequities, to a large degree, determine which children live and which ones die.
- Existing interventions can be implemented most effectively in countries where health systems work best.
- Child health programs in developing countries are grossly underfunded; major new investments will be needed in order to achieve the Goal.
Geographical distribution and causes of death
| A few diseases are responsible for the majority of childhood deaths | Some 10.8 million children are estimated to die before the age of five every year (Black, Morris, and Bryce 2003). Forty-one percent of these deaths occur in Sub-Saharan Africa, and 34 percent occur in South Asia. Just six countries account for half of all childhood deaths (table 3.1), and 90 percent of deaths occur in 42 countries. |
| Five diseases—diarrhea, pneumonia, malaria, measles, and AIDS—are responsible for an estimated 56 percent of deaths in children under five (table 3.2). In addition, about one-third of all deaths occur during the first month of life and have conventionally been grouped together as “neonatal deaths.” These have been attributed to a small number of biological conditions: complications of prematurity (27 percent), sepsis and pneumonia (26 percent), birth asphyxia (23 percent), and tetanus (7 percent) (Lawn and others 2005). These neonatal deaths have been relatively neglected in programs aimed at reducing child mortality and, for this reason, they are a special focus of this report. |
| Deaths from injuries are becoming proportionally more important | The imp... |