This is Volume XV of twenty-one in the Individual Differences series. Originally published in 1953, this study looks at the use of psychological tests in the practice of medicine when appraising personality. It is written primarily for doctors and psychologists, it is also directed towards social workers, clergymen, lawyers, teachers, counsellors, nurses, in short towards all who need to know more about the personality of those they work with in order to help them.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
As A GENERAL introduction to the new field of Clinical Psychology, we have imagined a conversation between classmates at a reunion. Physician Jones and Psychologist Smith meet after 20 years, and Jones, a general practitioner, catches up on this “newfangled profession” which he has been hearing about from some of his patients.
Physician: Hi, Smith – you're just the fellow I've been looking for. Heard of you from one of my patients the other day. Said she'd been to see you for some examination or other. What are you doing? You'd better bring my scanty knowledge of psychology up to date; from the little I took in college, I can't see any connection between its subject matter and the troubles of my hypertensive patient.
Psychologist: I can see what you mean. But academic psychology of 20 years ago was concerned with a totally different field of investigation and body of knowledge from what we now, as clinical psychologists, are interested in. Running rats through mazes, which you and I did in the old lab, differentiating between various degrees of brightness in experiments on visual acuity, demonstrating the size-weight illusion, learning nonsense syllables to demonstrate the laws of retention and recall – these admittedly are a far cry from the emotional problems with which we now deal professionally.
Physician: Glad to hear you say so. 1 was feeling baffled. Tell me, just what is this “clinical” psychology that you talk about?
Psychologist: The new profession of clinical psychology is slowly emerging as a recognized sociological entity, although the term was introduced as far back as 1896. It's a new job, created by the utilizing of new tools in dealing with human problems. We are only just beginning, amongst ourselves, to define our professional duties satisfactorily, to outline the training which we feel should be required of those who enter the profession, and to draw up an ethical code under the terms of which we will function. However, individual clinical psychologists have been working long enough and in enough places to have become part of the local framework of facilities available to persons in psychological distress, so I can give you a general picture of our activities.
Physician: I'm interested in that. In what way do you function in the assistance of the mentally disturbed? Is your province similar to that of a psychiatrist? Do you treat people or only examine them?
Psychologist: Let me begin at the beginning. I will talk about a hypothetical person, a composite picture of several of us who have gone into this field. A clinical psychologist gets his Doctor's degree in some branch of psychology. His basic, intensive, scientific training is not, as is yours or that of our psychiatric colleagues, in the field of the medical sciences. In addition to his major work in psychology, he will have, in all probability, done work in some allied field such as sociology, anthropology, and philosophy. Then he will have spent some additional years in the study of the specific tools, methods, and ways of investigating human personality. These methods have become known as the “projective techniques” and they are the instruments by which the psychologist provides information on the underlying motivations of the individuals he investigates. At the same time, he may have undergone a personal analysis and spent one or two years in close collaboration with his medical colleagues, either as an interne in some psychiatric or neurological hospital or in a clinic or guidance center where he will have an opportunity to relate his findings to the medical and psychiatric evaluation of the case.
Physician: Well and good, but I have a very concrete mind. I understand things better if I am presented with actual examples. Tell me about some of the patients you see, the reasons why they are sent to you, and in general what sort of things you can tell about them.
Psychologist: Well, that shouldn't be too difficult. Let me see – on Monday I spent the day testing a boy in his second year of medical school who had suddenly begun to do very badly in his studies.
Physician: You only saw one patient?
Psychologist: Sounds strange, I know, and it often surprises people because they do not realize how time-consuming the evaluation of the psychological material can be.
Physician: Do the tests take long to give?
Psychologist: The actual testing is not the most time-consuming thing. But the test material, when it has been accumulated, has to be evaluated and interpreted, and a report has to be written which gives relevant information to the referring physician. Testing two patients and writing two full reports would be a pretty heavy day's work. One could, of course, test several patients and write the reports at another time, but one has to allow from three to five hours for each case that is adequately tested, worked up and reported on.
Physician: Sorry I interrupted you. You were telling me about the young medical student.
Psychologist: Yes, it's a rather interesting case. He comes from a well-known family and was, you might say, all set for a brilliant career. When he began to do badly, there were enough persons with psychiatric orientation in his family so that he came very soon under the care of one of the best psychiatrists in the city, largely to discover whether or not some emotional disturbance was the cause of his sudden failure. The psychiatrist who was examining him, however, did not find any of the symptoms which might have been expected. He was referred for examination for whatever light could be thrown on his case by our test findings. In this instance, the psychological findings were very startling.
Physician: What did you find from the tests?
Psychologist: We strongly suspected from the findings that the boy's trouble arose from the fact that he had a slow-growing brain tumor, which, while it did not impair his overall intelligence, was affecting his creative thinking, his productiveness, and his capacity for abstraction to a marked degree.
Physician: You can tell that he has a brain tumor from your tests?
Psychologist: It is not quite as direct as that. We cannot tell with 100% certainty that he has a brain tumor. What we can point to is that some specific functions have been, as it were, knocked out, leaving others intact. The personality had acquired a stereotyped character, an impoverishment, a restriction of the psychological horizons which we have found to exist in patients with specific organic defects of the brain verified at operation. In this instance, my suggestion was, of course, that an electroencephalogram be done. The findings confirmed my suspicions. Let's see, I have the report here: “The electroencephalogram indicates that there is a focus of abnormally slow electrical activity appearing from the fronto-temporal region. This is regarded as presumptive evidence of a focal lesion in that region, most likely a brain tumor.”
Physician: Is that something which frequently happens in your practice? Surely not!
Psychologist: No, as a matter of fact, this finding is perhaps one in a thousand cases. However, a psychologist working in a neurological ward comes across this type of psychological finding frequently. In the ordinary run-of-the-mill of general practice, it is naturally very unusual.
Physician: What would have happened had there been no psychological examination?
Psychologist: Don't get the feeling that I consider myself indispensable in this connection. In this instance, however, it might have been easy to have overplayed the idea that some psychological disturbance was at the root of his trouble. This boy might have been put in treatment with some therapist on the assumption that his difficulties were basically emotional. He probably had emotional difficulties, as who does not? But I think the psychological tests may have saved considerable time since they highlighted so clearly that some organic condition was present.
Physician: Can you tell me what sort of things the test record, as you call it, of this boy showed?
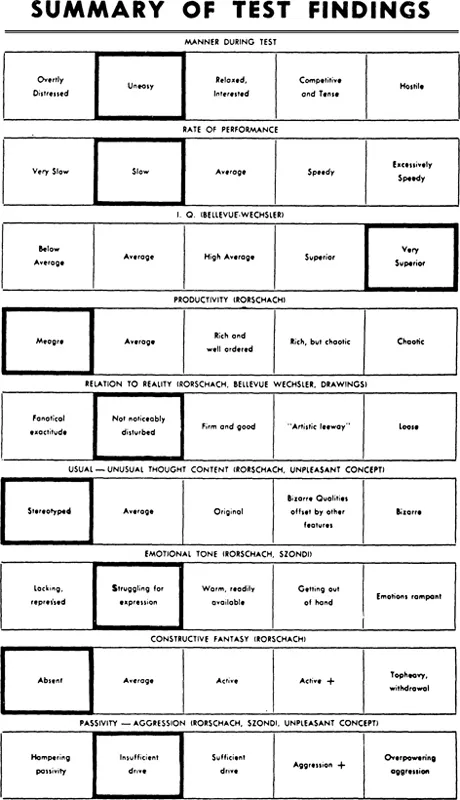
Psychologist: It would take too long at this point, old man; if you were really interested, perhaps you could drop into my office some time and I could show you some of the test material itself and tell you about it. The kind of technicality I could give you now would be meaningless, since you wouldn't have the background. However, I can show you a little chart that I use to summarize the test findings, which I think makes sense even if you don't know the tests themselves. I have devised this chart so that it would be possible for the physician to get a bird's-eye-view of how a patient reacted even though he does not know anything about the tests in detail. For example, take line one which describes in very general terms how the patient behaves during the tests. The boy I am talking about was somewhat “uneasy”. Patients who cry during the interview or whose anxiety over-powers them would have been recorded as “overtly distressed”At the other end of the scale would be the hostile patient who resents having to be tested and is angry at the examiner.
Then it is important to know about the rate of performance, how quickly does the person respond, how much does he deviate from the average, are there any unusual delays? It has been found that the individual whose responses come much quicker than the average is disturbed in a different way from the patient whose replies or responses are very slow. In the patient I am now describing, he was slower than the average.
The next line relates to the findings from a standard intelligence test. Here the range is from the “low average”up to “very superior”In this instance, our patient was found to have an I.Q. which fell in the Very Superior Group of the total population. This finding is important in the total diagnostic picture for some types of functions have been very well retained while others have been damaged.
Chart I Student with Brain Tumor
The next line relates to the patient's productiveness; productiveness, that is, in the same sense of his flow of spontaneous responses in one of the tests. This ranges from a “meagre”flow, on the one hand, to one which is rich and well-ordered or, and again in contrast, to one that is a chaotic production that has lost its richness. This will become more understandable to you as you are introduced in detail to one of the tests, the Rorschach inkblot test.
Our patient, in this instance, has a very meagrestream of associations. This despite the fact that he is very intelligent.
The line which is headed Relation to Realitywill also become more meaningful to you when the tests themselves are explained. Let me at this moment give you a simple illustration. I will draw the letter “H” and ask you whether I you will accept it as such. An individual whose relation to reality as shown in the tests, is one of what I might call “fanatical exactitude” would not accept this as an “H” because there is a slight discrepancy in the length'of the two parallel lines. An individual whose relation to reality is “not noticeably disturbed” or “firm and good” would, however, accept it. The individual whose test findings could be categorized as showing “artistic leeway” might say that this was not an “H” but a hurdle over which a runner had to jump. The individual, on the other hand, whose relationship to reality was “loose” might call this a dancing bear, that is, something which by all the ordinary laws of common-sense, there appears to be no connection whatsoever.
In dealing with the line entitled Usual or Unusual Thought Content, we can see that there is the possibility of extremely original thoughts being contrasted with those that are bizarre or those which show no originality whatsoever. Here again this particular patient shows no originality in his thinking which is interesting when one compares it with the fact that he is someone of a very superior intelligence. In other words, his originality and his spontaneous productivity have suffered while he is still “very intelligent.”
The line dealing with Emotional Tonevaries again from the possibility of expressing a lack of emotion on the one hand to an over-emphasis on the emotional aspects of life such that all else is obscured on the other.
The line headed Constructive Fantasyallows us the possibility of appraising an individual who has retreated into his fantasy completely, the schizoid individual, whose fantasy is, therefore, “top-heavy” and shows withdrawal symptoms. At the other end we are able to record an individual who is deficient in imagination, and in this particular case, imagination is another of the faculties which has suffered.
The final line relates to the extent to which the individual is too passive or over-poweringly aggressive.
Physician: That was interesting. Let's hear about another case, one of your more usual ones this time.
Psychologist: Yesterday I saw a husband and wife. I have made it a rule when there are marital problems and one member of the pair consults a psychiatrist who then sends him or her to me, that I do not make a report until I have seen the partner's psychological record also.
Physician: You insist that they both be examined even if only one is sick?
Psychologist: Yes. It has proved time and time again that it is almost misleading to examine one member of the discontented pair without the other. Or, let me say, the addition of the partner's record to one's understanding of the patient's complaints and difficulties adds so much as to make it almost imperative.
Physician: What was the trouble in the case you are speaking of?
Psychologist: In this instance, Mr. X consulted the psychiatrist with a list of what appeared to be perfectly genuine complaints about his wife's behavior. The man was unusually intelligent and convincing in his description.
Moreover, when the psychiatrist had an interview with the wife, he found her to have many of the characteristics of immaturity and childishness which her husband had described and which he considered an impossible barrier to their adjustment. As a matter of fact, when I saw Mrs. X and her husband, my impressions were entirely those which had been elicited by psychiatric examination. However, and it is here that the tests play their vital contributing part, while it is true that Mrs. X appeared childish, anxious, over-dependent, and emotionally immature on the tests which she took, and that her intelligence was a great deal lower than her husband's, as measured by our regular intelligence test scales–when her husband was examined, he proved, at the level to which the tests penetrate, to be much more seriously disturbed, although possessing an excellent facade or front. The husband, as a matter o...
Table of contents
Cover
Half Title
Title Page
Copyright Page
Table of Contents
List of Illustrations
Preface
Introduction
Part One
Part Two
Part Three
Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
Both plans are available with monthly, semester, or annual billing cycles.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go. Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Appraising Personality by Molly Harrower,Harrower, Molly in PDF and/or ePUB format, as well as other popular books in Medicine & Health Care Delivery. We have over 1.5 million books available in our catalogue for you to explore.