eBook - ePub
The Treatment of Shame and Guilt in Alcoholism Counseling
- 232 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Treatment of Shame and Guilt in Alcoholism Counseling
About this book
This insightful new book sheds light directly on shame and guilt--interactive aspects of the human condition that are deeply involved in the development and treatment of alcoholism and chemical dependency. Contributors to this valuable book discuss the process of healing internalized shame within the chemically dependent client and among the family members. They explore creative techniqes that foster understanding and coping strategies--videotaping and storytelling with clay and stuffed animals. Professionals who are experienced in treating chemically dependent clients and their families explore shame and the healing of shame, while examining the culture within which both occur. A major focus is the destructiveness of shame and guilt--shame keeps the family from seeking help, erodes self-worth, and produces destructive secrets that cannot heal, and guilt may circulate freely between alcoholic and family members, so that everyone begins to feel responsible for the pain of others.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Substance Abuse, Shame and Professional Boundaries and Ethics: Disentangling the Issues
Lindsay A. Nielsen, CCDP, SW
SUMMARY. The author addresses the special professional boundary concerns and ethics faced by therapists in their work with chemically dependent individuals and their families. Substance abusers and recovering chemically dependent counselors are identified as two populations especially vulnerable to boundary inadequacy. Included is a continuum which illustrates professional boundary issues/boundary violations, and recommendations for both the prevention and intervention of boundary violating behavior.
INTRODUCTION
The discussion of professional boundaries and ethics is crucial when exploring the process of shame for recovering chemically dependent people. There are a number of relevant issues to consider. The experience of guilt and shame is an inherent consequence of boundary violation, regardless of the nature of the relationship or the severity of the violation (Nielsen, 1984, 6–10; Coleman & Colgan, 1986). When the violator is someone in an authoritative role, the intensity of the shame for the victim often increases, as the victim is more likely to blame her/himself. It has been recognized that the process of substance abuse significantly alters boundary functioning, and that boundary inadequacy is widely found in chemically dependent families (Coleman & Colgan, 1986). The presence of boundary inadequacy leads to boundary violation, which is seen clinically in the higher rates of both childhood physical and/or sexual abuse, and current family violence patterns in the chemically dependent population (Nielsen, 1984, 6–10; Evans & Schaefer, 1987).
These issues are especially relevant for counselors as the therapeutic relationship greatly influences the restructuring of boundaries or the reinforcement of existing relational patterns. Professional boundary dilemmas are a normal part of the therapeutic relationship, but it is imperative that these be resolved appropriately for the client’s well-being, and for the well-being of the counselor and the organization. The process of professional boundary maintenance becomes more difficult if a counselor has problematic personal boundaries. Many recovering chemically dependent people, and recovering or nonrecovering adult children of alcoholics become counselors. These counselors may show significant personal boundary inadequacy which can lead to professional boundary violations.
Boundary issues are a necessary part of any counseling relationship. Some are easily handled but some are exceptionally complex. Questions of ethical concern are raised daily, often with conflicting answers. No counselor is able to therapeutically sort through all the issues in isolation.
It is also the hope of the author to challenge the notion that only “bad” counselors violate the boundaries of the clients, and “good” or competent counselors are not vulnerable. Counselors and therapists violate client boundaries for a myriad of reasons. “Neediness,” loneliness, personal crisis, lack of self-care, ignorance, and a history of victimization are all cited as reasons therapists exploit clients to meet their needs (Coleman & Schafer, 1986, 341–344; Schoener, 1984). Only a small percentage of offending therapists can be described as sociopathic or mentally ill. When we narrow the issues to good vs. evil, we miss the real issues which are relational. In most cases of boundary violations, clients experience great emotional turmoil due to conflicting feelings about the offender. In a shame-based philosophical framework (Good/Bad), we also lose the understanding and preventive possibilities offered by the use of a continuum.
Professional boundary dilemmas confront us daily, for they are part of a complex system of interacting. If we were to ascribe to the notion of “keep it simple” in this case, we would be forcing ourselves back into the language of shame: good/bad, wrong/ right, and easy/hard. We need to allow ourselves continuums, and the language of complexity.
DEFINING PROFESSIONAL BOUNDARIES
Professional boundary maintenance is the process of setting and maintaining boundaries specific to one’s professional role, taking into consideration all that accompanies that role. In counseling we need to assess our role, our client’s vulnerabilities and the nature of our particular therapeutic setting.
Consider the dynamics of a counseling relationship which differentiates these boundaries from other types of relationships:
- Clients enter the counseling relationship trusting us to act on their behalf at all times, simply by virtue of our role as counselor. This means that they assume we will make decisions that are in their best interest regardless of our personal situation, and regardless of whether we are “on duty” or “off duty,”
- The client enters the counseling relationship from a position of need.
- The client assumes the counselor is the expert, so will know better what is best for the client.
- Every counseling relationship involves the process of transference and counter-transference.
- All of these components interact to create a disparity of power. The counselor always has more power than the client. Due to this disparity of power the client never has true power of consent with the counselor. For example, even if the client initiated a romantic relationship, or if the client agreed to a sexual relationship with her/his counselor, this isn’t considered true consent.
Professional boundaries are built atop personal boundary structures. These professional boundaries are learned in a number of arenas. Professional boundaries and ethics are to date minimally taught in academic settings. Boundaries are also taught and modelled in clinical settings both from peers and supervisors. Law and ethical codes describe some ethical guidelines as does agency policy and formal and informal job descriptions.
Unfortunately for many clinicians, good training on professional boundaries and boundary violations has been all but absent from most of their training, academically and clinically.
Professional boundaries are also learned through experience. This learning tends to be more powerful than other types of learning. If a counselor (as a client) experiences serious boundary violations from another counselor, or a teacher, or a parent or other authority figure, then s/he is being taught both a behavioral system of boundary intrusions, and is also being taught the belief system which rationalizes the behaviors. If a counselor experiences appropriate boundary maintenance, this experience will also be translated into training for the role of counselor.
Every counselor has “blind spots,” some of which change with life circumstance. If a life situation closely parallels a client’s, there is a greater risk of boundary problems at that time. Boundary issues are clearly an integral part of the therapeutic process. In order for the counseling to be effective there must be trust, transference, care and concern. Boundaries play an integral role in all complex interactions, and boundary dilemmas and vulnerabilities will always be present. This author is in no way prescribing that the therapeutic relationship become a rigid, non-humanistic interaction of traditional psychoanalytic flavor. Resolving the boundary issues positively, in order to provide a healing experience, is crucial. Modelling healthy relational boundaries teaches skills in restructuring boundaries in other relationships as necessary. Given the generational nature of boundary inadequacy, this is imperative for our clients and their families.
Professional Boundary Violations
Defining professional boundary violations is more difficult than defining professional boundaries. A violation is different from a boundary issue. Boundary issues are a necessary part of the therapeutic relationship. Professional boundary violations are those boundary issues that when not appropriately addressed, become harmful to the client, or refer to those boundaries which should never be crossed by a counselor.
It is helpful to conceptualize therapeutic boundary issues and violations on a continuum. The existing literature clearly shows that severe professional abuses, such as a counselor having sex with a client, is often the final stage in a series of less severe violations (Coleman & Schaefer, 1986, 341–344; Nielsen, Peterson, Shapiro & Thompson, 1986). Boundary problems can be defined as all of the beliefs and behaviors exhibited by the counselor that in some way move the client from client status while s/he maintains client vulnerability.
As has been shown with familial incest (Evans & Schaefer, 1987; Nielsen, 1984, 6–10) the underlying belief system and preceding emotional and psychological violations are often just as harmful as the “overt” behaviors. This concept also applies to professional boundary violations. Consider the following continuum for professional violations.
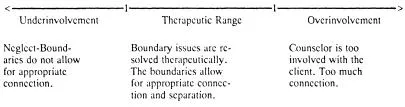
Counselors can exhibit boundary problems that fall into the category of neglect or underinvolvement. Failure to return phone calls, indiscriminately cancelling sessions, nor paying due attention to the therapeutic needs of clients, failing to acknowledge the emotional connection between themselves and their clients, failing to say goodbye appropriately, etc., are all examples of neglectful boundaries or underinvolvement. Clients who are neglected will experience all of the consequences of boundary violations, just as from those of overinvolvement. neglect is inherently shaming. Clients question what they did wrong, and why they’re not important enough to warrant attention.
The therapeutic range includes boundary issues and dilemmas. The counselor is appropriately involved with the client. There is a therapeutic balance between separation and connection. The generational boundaries are clear. The counselor doesn’t abdicate his/her role, and the needs of the client are appropriately weighted and addressed.
In the overinvolved range there is too much connection. The needs of the client are not appropriately focused on. The counselor may attend only to the client’s needs for connection without therapeutically balancing with the client’s needs for separation. The counselor abdicates her/his role as s/he moves the client out of client status. Some examples of severe violations include: accepting expensive gifts from a client, borrowing money from a client, physically assaulting a client, or being sexual or romantic with a client. All of these situations fall on one extreme end of the continuum of boundary violations. While few counselors would argue that these are boundary violations, they still occur with frightening frequency.
Between 10–17% of the counselors researched admitted having sex with one or more clients (Kardener, Fuller & Mensh, 1973, 1077–1081; Brudsky, 1986). This statistic is probably conservative and doesn’t include severe violations of a nonsexual nature. Fifty percent of the psychiatrists surveyed by Grunebaum, Nadelson, and Macht, stated that they knew of cases where a therapist was being sexual with one or more clients or patients. Few had reported the situation. These statistics don’t include situations involving “former” clients or patients. The...
Table of contents
- Cover
- Half Title
- About the Editors
- Full Title
- Copyright
- CONTENTS
- Shame in the Eighties
- Shame and Guilt: Definitions, Processes and Treatment Issues with AODA Clients
- The Process of Healing Shame
- Creative Approaches to Shame and Guilt: Helping the Adult Child of an Alcoholic
- Rekindled Spirit of a Child: Intervention Strategies for Shame with Elementary Age Children of Alcoholics
- Videotaping in Groups for Children of Substance Abusers: A Strategy for Emotionally Disturbed, Acting Out Children
- From Guilt Through Shame to AA: A Self-Reconciliation Process
- Substance Abuse, Shame and Professional Boundaries and Ethics: Disentangling the Issues
- Shame and Guilt Issues Among Women Alcoholics
- Shame, Boundaries and Dissociation in Chemically Dependent, Abusive and Incestuous Families
- Shame and Forgiving in Alcoholism
- Measuring Shame: The Internalized Shame Scale
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Treatment of Shame and Guilt in Alcoholism Counseling by Ron Potter-Efron,Patricia Potter-Efron in PDF and/or ePUB format, as well as other popular books in Psychology & Addiction in Psychology. We have over 1.5 million books available in our catalogue for you to explore.