eBook - ePub
The Occupational Therapy Managers' Survival Handbook
A Case Approach to Understanding the Basic Functions of Management
- 221 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
The Occupational Therapy Managers' Survival Handbook
A Case Approach to Understanding the Basic Functions of Management
About this book
This practical volume, in a casebook approach, was developed in response to the complex issues that today's manager faces. As therapists assume managerial responsibilities, there is need to share experiences and lessons learned. In this volume, a common format is used to present each case, including chronology of events, alternatives considered, risks involved, and outcomes. Several chapters include valuable resource materials as well. Key concerns are addressed, such as justifying more therapist staff, evaluating staff performance, collecting and analyzing cost data to establish fees, weighing ethical and liability concerns, and teaching students about their future responsibilities. The Occupational Therapy Manager's Survival Handbook provides useful material for any therapist who wishes to examine and strengthen his or her role as a manager.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Health Care DeliveryThe Development of a Fee Structure for Productivity Analysis and Program Management
Marilyn Dennis,MPA,OTR
Lana Ledet,OTR
SUMMARY. Occupational therapists are frequently promoted to management level positions without prior instruction in financial accounting. Accounting information can enhance rational decision making processes at both the middle management and supervisory levels. Although today's literature encourages health care professionals to utilize accounting principles, the occupational therapy manager is often uncertain as to how to apply these techniques to his own setting.
This paper describes how one multiclinic department revised its existing fee structure and utilized the generated data to analyze ther-apists' productivity and to effect decisions regarding program management.
OVERVIEW
A large occupational therapy department had a change of directors and other significant personal within a six month period. The director was confronted with the problem of reducing costs, while maintaining quality of care, enhancing productivity and developing a more judicious distribution of the 44 therapists and their assignments in a multiclinic department. This paper will describe the events related to the implementation of a relative value unit system for determining fees and staff productivity, an analysis of the data generated, and a description of how the outcomes of the productivity analyses were used for program decision making.
THE PARTICIPANTS
The primary author had just joined the department to supervise the physical dysfunction section. Because of her graduate training in public administration, and some previous experience in evaluating productivity in a smaller department, she was asked to develop a comprehensive charge system. The second author, meanwhile, had begun to develop skills in computer use. The two therapists combined efforts to develop a new charge system and a computer program to analyze the data generated by 44 therapists.
THE ORGANIZATION
The occupational therapy department is housed in a state medical university. The department director reports to an executive director for professional services of the university hospital. Occupational therapy is relatively autonomous in decision making. There are two assistant directors administering two distinct divisions: one in the physical dysfunction area, and the second in psychiatry and pediatrics. A leveling system provides recognition of staff's administrative and or clinical expertise; staff members may be designated as I, II, or Ill's contingent upon responsibilities and qualifications. Twelve occupational therapy clinics are geographically scattered throughout the 64 acre campus.
CHRONOLOGY OF EVENTS
In September of 1985, the director of occupational therapy expressed an interest in revising the existing fee structure and improving upon the means then available for therapists to document productivity. There were three essential functions involved in the process. The first consisted of revising the charge system based on data compilation, financial and staff accountability. The second function required data manipulation and analysis through the use of computer technology. The third and final function is an ongoing process requiring those in administration to make decisions based on the data which is compiled and analyzed monthly.
CONTEXT
Upon reviewing the existing charge mechanism, it was intended that the new system address several issues:
1. Charge categories that more appropriately described services rendered were needed to improve the department's ability to recover costs. The existing system listed only five service categories in which to describe treatment given. Treatment time could be charged in one quarter hour up to one hour units but time in excess of that was not being charged (Figure 1).
2. No means existed to differentiate the charges for a simple versus a complex treatment and/or evaluation. For example, a treatment in reality orientation would be billed under Physical Medicine and Rehabilitation at the same charge per time unit as a neuromuscular treatment. Reality orientation can often be performed by a COTA while a neuromuscular treatment may require the expertise of a therapist certified in NDT.
3. Uniform description of charge categories, adaptive equipment, and splints was also necessary to increase potential for third party payor reimbursement.
4. A procedure to allow therapists to charge for adaptive equipment lprovided to patients was critical. The existing structure did not offer this and equipment items were given to patients with no means of recovering costs to the department.
5. Reimbursement for occupational therapy services offered in psychiatry was a primary concern. The existing system did not allow for patient charges to be generated from that service area although one third of the occupational therapy staff were employed in this clinical area.
6. Group treatment charges were unavailable with the existing charge structure. The majoriity of psychiatric treatments were conducted in groups and thus required a lower fee per patient.
7. A more accurate reporting system for individual therapists, teams, and divisions to assess billable time was essential. This specific information would assist in determining plans for program development and more efficient assignment of personnel to teams. It would also increase administration's awareness of frequency of services rendered according to type of treatment, i.e., homemaking, neuromuscular; and group versus individual treatment as it related to various OTRs, COTAs, teams, and divisions.
Although the department is in a teaching hospital setting, and there are many demands on therapists beyond patient treatment (i.e., administrative tasks, clinic teaching, research and program development), therapists had not reached an adequate level of billable productivity (therapist time which can be charged to the patient, i.e., treatment preparation, direct patient care, documentation, travel time, and chart review). With the existing fee structure, departmental expenses were not being met. Also, the staff average daily treatment units did not match that of comparable departments elsewhere.
An unfortunate clinical reality is that however important some functions might be, not all of the therapist's functions are billable In this particular department, nonbillable or indirect patient care tasks had consisted of: performance of administrative tasks, student supervision, nonchargeable patient related activities such as scheduling, ordering equipment for the patient, and discussing patient's status informally with other disciplines, developing new programs,
EXISTING CHARGE SLIP — 1984
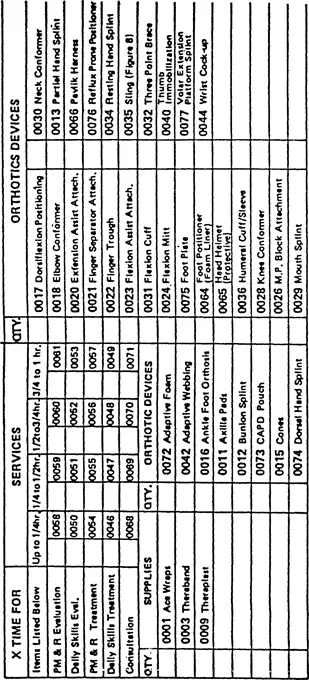
Figure 1
providing assistance to another therapist during patient treatment, and transportation of patients to and from clinics due to lack of an aide. It was apparent to administration that not only were these functions valid and deserving of recognition, but several tasks displayed reimbursement potential as well, i.e., ordering equipment for patients, and transportation of patients to and from the clinics. Thus, the challenge existed to create a vehicle for acknowledging their value. Changes were needed in both the fee structure and documenting procedures.
CHOICES
After deciding that a revised charge system was needed, the literature was reviewed to obtain guidelines for charges in occupational therapy. In 1970, Mae Hightower-Vandamm suggested three philosophies for development of fees for service. First was the philosophy that encouraged the availability of occupational therapy for all who need it regardless of costs. Second was the proposal that occupational therapy charges should be in accordance with those in physical therapy. The third proposal encouraged the use of comparable rates charged in the community. Although the first is altruistic, it does not contain costs. With the second approach, the treatment modalities in physical therapy and occupational therapy vary extensively and no longer offer a practical means to develop fees. And although surveys of fee schedules of hospital departments within the community are necessary to assure a competitive market, such a technique does not assure that expenses will be met and/or that a profit margin will be achieved.1
Laase describes two types of pro...
Table of contents
- Cover
- Half Title
- Full Title
- Copyright
- Contents
- ABOUT THE EDITORS
- FROM THE EDITOR'S DESK
- FROM THE CO-EDITOR
- Justification of Staff Positions in a Tightening Marketplace
- Occupational Therapy Staff Evaluation: A Personnel and Program Management System
- The Development of a Fee Structure for Productivity Analysis and Program Management
- Conflict Management: A Study of Alternative Approaches
- Personnel and Human Resource Management in the Occupational Therapy Curriculum
- The Occupational Therapist as a Consultant: A Model of Community Consultation
- Marketing: A Reasonable Administrative Approach to Decision-Making
- Ethical and Professional Liability Considerations for the Administrator: Incidents and Principles
- Administrative Considerations in Designing and Implementing Changes in Occupational Therapy Programs
- Developing and Implementing an Interdisciplinary Feeding Training Program Within a Large Institution: The Manager's Planning Responsibility
- A Database Approach to Managing an Occupational Therapy Department
- PRACTICE WATCH: THINGS TO THINK ABOUT
- BOOK REVIEWS
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access The Occupational Therapy Managers' Survival Handbook by Florence S Cromwell,Chestina Brollier in PDF and/or ePUB format, as well as other popular books in Medicine & Health Care Delivery. We have over 1.5 million books available in our catalogue for you to explore.