Tavistock Press was established as a co-operative venture between the Tavistock Institute and Routledge & Kegan Paul (RKP) in the 1950s to produce a series of major contributions across the social sciences.
This volume is part of a 2001 reissue of a selection of those important works which have since gone out of print, or are difficult to locate. Published by Routledge, 112 volumes in total are being brought together under the name The International Behavioural and Social Sciences Library: Classics from the Tavistock Press.
Reproduced here in facsimile, this volume was originally published in 1976 and is available individually. The collection is also available in a number of themed mini-sets of between 5 and 13 volumes, or as a complete collection.
- 424 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
An Introduction to Medical Sociology
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicinaPart I

Introduction
Chapter 1
Introduction
It is now some years since the official bodies that control medical education in the UK recommended that all medical students should pursue studies of sociology (General Medical Council, 1967: 15; Royal Commission on Medical Education, 1968: 104–9). Over the last few years it has become commonplace for these students, as well as for many doctors with long experience in clinical work, to take some kind of sociology course. Yet to many of those required to follow sociology courses, and indeed to many of those who have required students to do sociology, the subject is something of an obscure mystery – often considered to have some relationship to socialism or to social work. In this chapter I want to consider some of the features of present-day medical practice that have led to the inclusion of sociology as a useful preparatory discipline and then go on to introduce some of the sociological concepts I consider salient to medical practitioners. Finally, I will review some of the issues in medical practice that I believe can be illuminated by sociology.
But first I should issue a warning: in some respects sociology may be frustrating to the would-be practitioner. Whereas the medical student, particularly at an early stage of his career, wants cut and dried answers, recommendations, and solutions, he will find that the sociologists writing in this book seem to provide only questions, complications, and ways of looking at medical practice. In this respect the sociologist’s approach may be rather different from those he experiences in many other subjects. Nonetheless, I believe it to be profoundly useful. Through greater sociological understanding many clinical judgments may be made more rationally; much of the frustration in present-day practice may be overcome; the behaviour of patients, of colleagues, and of large organizations may be better appreciated; and the doctor may be able to exercise the therapeutic skills he has learnt in other parts of his training more effectively for the benefit of his patients. Wherever possible, the authors will try to indicate how we think sociology can be useful. But inevitably clinical practice consists of individual cases and each doctor has to learn how to use sociology to his own, and to his patients’, advantage – just as he must decide how to apply the other knowledge he has gained in his training.
Some Changes in Medical Problems and Medical Practice
There are about 55,000 doctors employed in the National Health Service. About half of these doctors work in the community – the majority as general practitioners, but a few in the administration of the health, education, and social services, and a few more in industrial settings. About 11,000 doctors work as consultants providing specialist medical care in NHS hospitals, and about 19,000 others assist them as ‘junior hospital doctors’ in various stages of their apprenticeship (although not all such doctors ultimately become consultants) (Department of Health and Social Security, 1974a: 28).
Up to the present, regardless of the specialty or part of the health service that they will eventually work in, all doctors have a common undergraduate training. To a large extent this training concentrates on providing students with the basic scientific knowledge and clinical experience to diagnose quickly and accurately acute life-threatening disease. A student learns to recognize the signs and symptoms of those diseases for which medical science has an available treatment – the infectious diseases, acute appendicitis, trauma, some cancers, and so on. There is an obvious logic to this emphasis in training: when a student starts to practice without supervision the failure to recognize the appropriate signs and symptoms of acute, life-threatening disease would be immediately and unnecessarily fatal to his patients.
But an analysis of the types of conditions that doctors are now called upon to treat – whether in the hospital or as a general practitioner in the community – suggests that this kind of acute life-threatening illness, and the emphasis on speed and accurate diagnosis which it necessitates, is no longer a major part of most doctors’ work. The very success of medical technology – notably the development of antibiotics, and the still more significant advances of preventative medicine – coupled with the rise in living standards, has dramatically reduced the significance of infectious disease. Smallpox, for example, was once the major killing disease. Now, in almost every country in the world, it is an unusual event and is seldom fatal. The present pattern of disease means that doctors are now mainly called upon to treat conditions that prevent individuals from performing self-supporting activities or from developing the intellectual and physical potentialities needed to achieve an inner sense of well-being – that is, conditions like chronic rheumatism and arthritis, chronic bronchitis, diabetes, epilepsy, anaemia, multiple sclerosis, and various forms of mental ‘difficulties’. With these kinds of diseases the main danger is not that inadequate practice on the part of the doctor will lead to the patient’s death, but that it will lead to unnecessary suffering, discontent, inconvenience, or humiliation. Furthermore, since modern medical techniques often keep alive a patient who in earlier times might have died, the doctor now has to help a patient react to and cope with the handicaps that the onset of a condition may impose. [1]
An analysis of the usage of English hospital beds in 1972 gives some indication of the type of conditions doctors are now called upon to treat. Table 1, for example, shows how 30 per cent of all beds in non-psychiatric hospitals are taken up by individuals aged over seventy-five and that 50 per cent of all beds are taken up by individuals over sixty-five. If we look at female patients alone, and exclude those in hospital for maternity care, we find that nearly two thirds of all beds are taken up by individuals over sixty-five. The conditions that these older age groups suffer from are very largely of the degenerative chronic type – quite different to the acute, life-threatening disease of the past.
Table 1 Percentage of beds occupied in non-psychiatric hospitals in England by different age groups
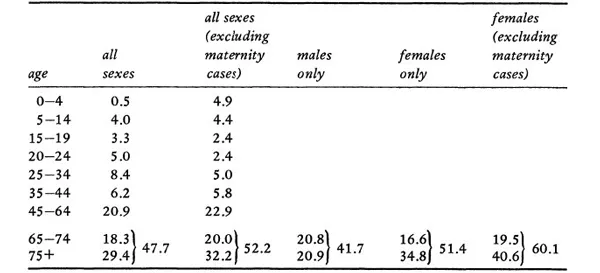
Source: Specially compiled by Dr John Ashley (of the London School of Hygiene) from information supplied by the DHSS in 1-patient enquiry (DHSS, 1974b). (See Klein and Ashley, 1972.)
The department of Health’s Hospital In-Patient Enquiry (1974b) provides details of a bed-census carried out in all English non-psychiatric hospitals in 1972. Table 2 provides information on the most frequent diagnoses given on patients in hospital in 1972. The left-hand column gives a picture of the hospital population at any one moment – the individuals you could encounter in a walk around hospitals on an average day – and the right-hand column shows the number of discharges or deaths. Where there are differences these reflect the length of stay required for different conditions. From the table it can be seen that the major categories in terms of bed occupancy are: malignant neoplasus (7 per cent); strokes (9 per cent); arterial disease (3 per cent); childbirth (9 per cent); arthritis (4 per cent); and fractures (5 per cent). The great majority of these conditions are ones which have long-term implications for treatment and management. Infectious diseases, it will be noted, hardly figure at all.
Table 2 Bed occupancy and admissions in non-psychiatric hospitals in England 1972* (All conditions over 1%)
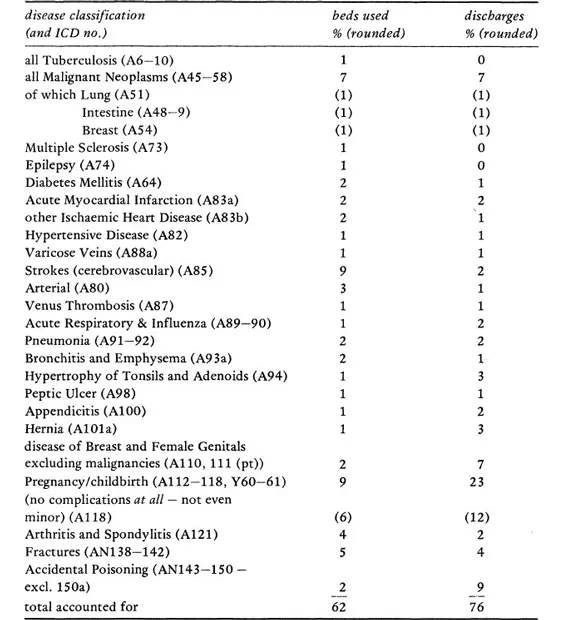
(Source: DHSS, 197413: Table 6)
* I am grateful to Dr John Ashley of the London School of Hygiene for help and advice in the preparation of this table.
All the figures reported above refer to non-psychiatric hospitals, which themselves account for about half of all hospital beds. The number of psychiatric beds, therefore, is very large. The age distribution for psychiatric bed usage is very similar to that in non-psychiatric hospitals and the vast majority of psychiatric in-patients fall into the chronic category – patients whose conditions are treated and managed, in and out of hospital, over long periods of time. About one third of all psychiatric beds are taken up by patients who are mentally subnormal or mentally handicapped, while the remaining two thirds are taken up by patients suffering from some form of ‘mental’ illness (DHSS, 1974a: 152 and 127).
The picture is even more clear in general practice. The average general practitioner with 2,500 patients on his list will spend between 6–17 percent of his time dealing with acutely ‘serious’ disease of a life-threatening variety. He will spend somewhere between 51/77 per cent of his time treating ‘minor’ diseases and between 8–30 per cent of his time managing ‘chronic’ complaints (Backett et al., 1954; Brotherston et al., 1959; Eimerl, 1960; Fry, 1966; Wright, 1968; Williams, 1970). The types of disease that the general practitioner sees in the various categories are set out in Tables 3–6.
Table 3 Estimates of severity of disorders seen in general practice expressed as percentages of total consultations
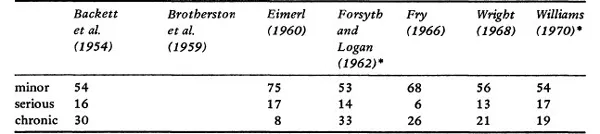
Source: Royal College of General Practitioners (1973: 19)
* adapted: recorded under physiological, trivial, acute serious, acute non-serious, chronic serious, and chronic non-serious
Table 4 Acute major illness (life-threatening)
illness | persons consulting |
pneumonia and acute | per year |
bronchitis | 50 |
acute myocardial | |
infarction | 7 |
acute appendicitis | 5 |
All new cancers | |
lung | 1–2 per year |
breast | 1 per year |
large bowel | 2 every 3 years |
stomach | 1 every 2 years |
bladder | 1 every 3 years |
cervix | 1 every 3 years |
pancreas | 1 every 4 years |
ovary | 1 every 5 years |
oesophagus | 1 every 7 years |
brain | 1 every 10 years |
uterine body | 1 every 12 years |
lymphadenoma | 1 every 15 years |
thyroid | 1 every 20 years |
severe depression | 12 |
suicide | 1 every 4 years |
attempted suicide | 2 every year |
acute glaucoma | 1 |
acute strokes | 5 |
killed in road accident | 1 every 3 years |
Source: Royal College of General Practitioners (1973: 30)
Table 5 Minor illness (of short duration and minimal disability)
illness | persons consulting |
upper respiratory infections | 500 |
common gastrointestinal ’infections and dyspepsias’ | 250 |
skin disorders | 225 |
emotional disorders | 200 |
acute otitis media | 50 |
wax in external meatus | 50 |
‘acute back’ symptoms | 50 |
migraine | 30 |
hay fever | 25 |
acute urinary infections | 50 |
Source: Royal College of General Practitioners (1973: 19)
Table 6 Chronic illnesses
illness | persons consulting |
chronic rheumatism | 100 |
rheumatoid arthritis | 10 |
chronic mental illness | 55 |
severe subnormality | 5 |
educationally subnormal | 3* |
vulnerable adults | 40 |
child guidance | 4* |
chronic bronchitis | 50 |
anaemia | 40 |
pernicious anaemia | 2 |
hypertension | 25 |
asthma | 25 |
peptic ulcer | 25 |
strokes | 15 |
epilepsy | 10 |
diabetes | 10 |
Parkinsonism | 3 |
multiple sclerosis | 2 |
pulmonary tuberculosis | 2 |
chronic pyelonephritis | 1 |
Source: Royal College of General Practitioners (1973: 20)
* persons attending school or clinic
From these tables it can be seen that the ‘real’ disease of medical school education is quite rare – a GP, for example, only sees a case of lung cancer, the second most common form of death in the UK, once or twice a year. Even acute myocardial infarction will only be encountered about seven times. To summarize, the great majority of the cases the GP sees are either ‘trivial’ or ‘minor’ in a medical sense and tend to be chronic either in their course or in their implications. Myocardial infarction, for example, although acute in its course, has long-term implications for the patient’s life and medical management. As a result, therefore, of present patterns of health and disease or, more strictly, patterns of the demand of individuals for the doctor’s help, today’s practicing doctors, both in hospital and in general practice, are as often concerned with the long-term management as they are with the immediate cure of disease.
In modern conditions the management of disease is infrequently a matter of the indiv...
Table of contents
- Cover Page
- Half Title page
- Series page
- Title Page
- Copyright Page
- Original Title Page
- Original Copyright Page
- Contents
- Acknowledgements
- Preface
- Part I Introduction
- Part II Background
- Part III Areas of Medical Sociology
- Part IV Conclusion
- Name Index
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access An Introduction to Medical Sociology by David Tuckett in PDF and/or ePUB format, as well as other popular books in Medicina & Prestazione di assistenza sanitaria. We have over 1.5 million books available in our catalogue for you to explore.