This book is destined to become a classic in its field.
Sidney Sax, Chairman, Ethics Committee, Australian Institute of Health and Welfare, former Director of Health Services, Planning and Research, NSW
The whys and hows are clearly and carefully explained for everyone involved in planning health services of all sizes in today's demanding climate. No health planner should go to work without this book.
Tony Adams, Professor of Public Health, National Centre for Epidemiology and Population Health, Australian National University
Increasing concern about a positive return on investment in health leads to a need to make choices. As a result, skills in planning are increasingly being required of managers, providers and policy makers in health care.
Experienced planners and teachers Kathy Eagar, Pamela Garrett and Vivian Lin have written a comprehensive introduction that bridges the theory and practice of health planning. They outline the health policy and planning context, the impact of different resource allocation environments on planning, and explain the processes and the technical skills needed to undertake service, program, corporate, business and facility planning.
The authors also explore major challenges facing health planners, including the growing role of market forces in health care, the need to balance equity of access with equity of outcomes, and the tension between planning for population health versus planning for more efficient health care delivery.
Illustrated with extensive case studies from both the public and private sectors, Health Planning is an indispensable reference for health professionals and a valuable text for students.
- 448 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
PART I
OVERVIEW AND CONTEXT OF HEALTH POLICY AND PLANNING
1 INTRODUCTION TO HEALTH PLANNING
Since the Second World War, governments in Western industrialised countries have engaged in the planning of health services (Rodwin 1984). Health planning institutions and approaches have varied, but they have shared a common range of concerns. These include:
- How should health needs be assessed and met?
- How should a health system be organised and financed?
- What is the appropriate role and scale of hospitals? and
- What are the appropriate responsibilities for public health programs?
Over the years the focus of health planning effort has changed. Health planning has evolved from the post-war expansionary phase to issues of cost containment and now to a concern with accountability and health outcomes. The early successes of creating a ‘medical–industrial complex’ have led, ironically, to a need to critically examine issues of effectiveness, efficiency and equity.
This chapter introduces the main theoretical issues and debates pertaining to planning in general and health planning specifically. It describes the different ways in which planning is conceived and practised. Definitions of key terms are provided. The fundamental dilemma of planning — whether to plan for health services or to plan for health improvement — is also raised.
WHAT IS PLANNING?
Planning can be thought of in numerous ways and is applicable to numerous activities. Most people try to arrange ahead many of the events of life. Budget planning is concerned with the allocation of limited and finite financial resources. Town planning is concerned with the control of influence on the future pattern of urban development and urban services. Most countries — at the national, state or local levels — engage in national security planning, economic planning, social planning, environmental planning and regional development planning (Friedmann 1987). Dictionaries typically define the verb ‘to plan’ as meaning ‘to arrange the parts of’, ‘to realise the achievement of’ or ‘to intend’. In the colloquial sense, then, ‘planning’ is concerned with deliberately achieving some objective by assembling actions into some orderly sequence.
Green (1999) suggests that planning, as a separate identifiable activity in organisations, emerged from three strands of development. First, the rise of modern, complex industrial organisations in the late nineteenth century required decisions about the future to be taken in a considered and explicit manner. Second, the Russian Revolution of 1917 led to the attempt to build an economy based on nationally determined plans and, hence, to the need for formal state planning (and planning bureaucracies). Third, the shortages experienced during the Second World War led to centralised controls in many Western countries.
In Western industrialised democracies, planning as a generic activity and as a profession is commonly identified as emerging in the twentieth century, particularly after the Great Depression of the 1930s. Planning evolved as an attempt to mitigate the negative consequences of a laissez-faire market economy that was characterised by unrestrained pursuit of self-interest by individuals and corporations (Friedmann 1987). The idea was for the state to intervene in markets through planning instruments in order to protect the collective interest. Public planning has thus had a long association with the notion of the welfare state and it has often been seen to be in conflict with private interests.
Definitions of planning often reflect a tension between the technical tasks undertaken by the profession and the end objectives to be achieved by the tasks. In a generic and technical sense, planning can be conceived of as:
- ‘the process of preparing a set of decisions for action in the future, directed at achieving goals by preferable means’ (Dror 1973, p. 330); or
- ‘making current decisions in the light of their future effects’ (Reeves and Coile 1989, p. 2).
However, ways of thinking about planning have evolved with changes in society and the economy. In the 1940s, planning was concerned to set up the desired future end state in detail (that is, blueprint), but by the 1960s planning concentrated on the objectives of the plan and ways of obtaining them or systems planning (Hall 1992). Hall suggests that, in the 1970s, planning became more heterogeneous and diffuse, and it could be characterised as continuous participation in conflict. Friedmann (1987) would emphasise that planning, as the application of technical reasoning to specific problems and leading to action or policy intervention, occurs in a social and political context.
Mainstream planners typically work for the state, although increasing numbers also work within civil society. The planning profession has historically seen the discipline as ‘basically a methodology, a set of procedures applicable to a variety of activities aimed at achieving selected goals by the systematic application of resources in programmed quantities and time sequences designed to alter the projected trends and redirect them toward established objectives’ (Robinson 1972). Such a perspective emphasises the technical and rational aspects of planning. Taylor and Reinke (1988, p. 5) expand on this perspective when they agree that ‘effective planning requires stepwise application of selected multidisciplinary methods and procedures to designated programs and projects within specified time frames’. They add that ‘planning is not simply a technical exercise; it is an ongoing process of learning, adapting to change, and educating’.
As planners move into positions of facilitating change, the traditional model of rational planning is inserted into, if not transformed by, political practice. The values inherent in planning are made explicit by Blum (1974). Planning, he says, ‘is devoted to directing and attaining social changes of a specific and desired nature’ and is the ‘preferred means of achieving deliberate change’ (p. 14). Friedmann (1987) also sees planning practice as linking scientific and technical knowledge to processes of societal guidance, if not social transformation. In the ‘societal guidance’ model, planning is articulated through the state and is concerned with systematic change, while the political practice of system transformation becomes the focus on planning practice concerned with social transformation.
Parston (1980) suggests that planning is both an occupation and an idea. As an occupation, planning is work, a job. As an idea, planning is ‘a process which is undertaken to meet some desired objective or to fulfil some purpose’ (p. 23). He argues they are inseparable. Forester (1982) also sees an activist role for the planner, in that planners are not only involved in problem solving; they are also concerned with problem finding or the mobilisation of attention to issues of concern.
WHY PLAN?
As an activity that all organisations carry out with a greater or lesser degree of explicitness, planning involves making choices. When carried out by the public sector, planning is often conceived of as an intervention in the free market. In theory, the market allows equilibrium to be established between supply and demand as resources move in response to price signals. State intervention is limited, and ‘non-market goods’ are produced in a complementary public sector. Classical economists see the market as the most efficient means of operating an economy. However, certain key conditions have to be met. These include good knowledge by the purchaser (or consumer) of the goods or services on offer, buyers and suppliers operating independently, and the market operating independently to the extent that a purchase by one consumer does not necessarily affect the decision by another to purchase.
Planning, as an instrument of state intervention, has been justified on a number of grounds since the second half of the twentieth century. Milton Friedman, an economist who champions the free market, supports state intervention in the presence of natural monopolies and externalities. The liberal perspective (such as espoused by Galbraith, Titmus, Lindblom and Musgrave) suggests that state intervention is justified in order to correct market failure, to redistribute income, and to manipulate fiscal and monetary policies in order to affect aggregate demand. Structuralist critiques of the state (such as those by Habermas, O’Connor and Offe) suggest that the contradictory need to maintain the conditions for capital accumulation and to raise revenue to meet its own obligation creates the need to convey an image of pursuing common and general interests of society as a whole, allowing access to power and responding to justified demands.
Planning has also been more recently criticised for its utilitarianism. Modern statecraft has been described as ‘devoted to rationalising and standardising . . . a social hieroglyph into a legible and administratively more convenient format’ (Scott 1999, p. 3). State planning schemes can be seen as a means of social engineering, greater regimentation of communities and daily lives, and enhanced state capacity.
Different conceptions of the role of the state will drive views on the nature and extent of state intervention required. For the health sector, views on the need for, and the nature of, state intervention depend on whether the state is seen as regulator, service provider, financier or policy formulator for the health sector. In relation to health planning as a form of state intervention, the promarket position argues that health planning is likely to increase administrative controls and reduce professional autonomy and consumer choice. Health services delivery systems based on a professional model or a competitive free enterprise model (such as in the United States) would be favoured. The radical critique, in contrast, would see health as a right rather than a commodity, and would prefer distribution of health resources on the basis of need. A model that requires central planning and regionalisation of health resources, such as the National Health Service in England prior to the Thatcher reforms, would be favoured. A mid-way position, represented by liberals, would accept a mixed system of public and private service provision and financing, and focus state intervention on criteria such as accountability, rationality and equity.
Irrespective of their ideological positions, all governments ultimately need to make allocative decisions. As shown in Figure 1.1, allocative decisions are required across various sectors as well as within the health sector.
Given that pure markets do not exist in the Australian context and that public sector financing and provision are dominant features, the setting of health care priorities is largely determined through health planning. The question, then, is not whether health care should be planned, but what to plan, by whom, how and when.
PLANNING TRADITIONS
Friedmann (1987) classifies the intellectual traditions of planning theory according to their political ideology as well as the intended use of knowledge. He identifies four distinct tendencies, as shown in Table 1.1.
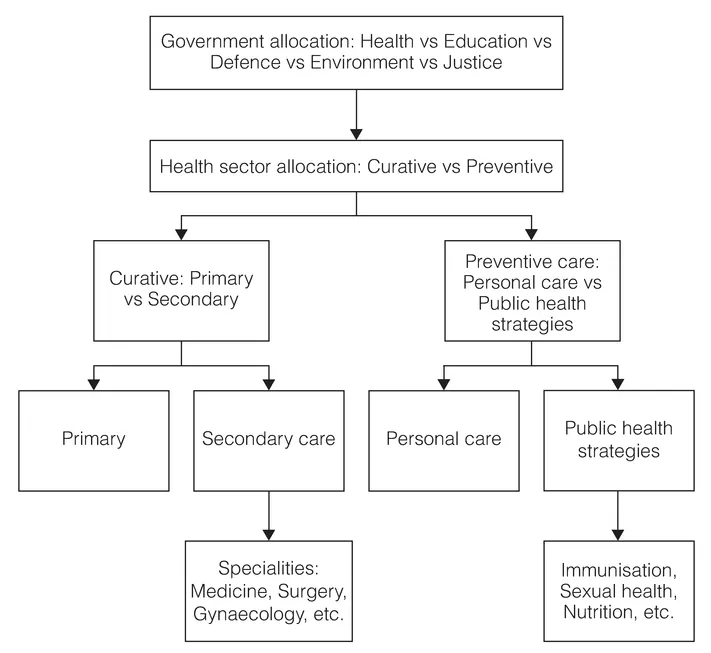
Figure 1.1Levels of allocative decision making by government
Source: adapted from Green 1999 p. 5.
The ‘policy analysis’ tradition (including Dror, Benveniste and Wildavsky) derives from organisational theory, particularly how large organisations might improve their ability to make rational decisions. It is a rational–technical approach which builds on public administration, sys...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Contents
- List of figures, tables and boxes
- Abbreviations
- Preface
- About the authors
- About the case study authors
- PART I OVERVIEW AND CONTEXT OF HEALTH POLICY AND PLANNING
- 1 INTRODUCTION TO HEALTH PLANNING
- 2 TRENDS AND ISSUES IN THE AUSTRALIAN HEALTH SYSTEM
- 3 A BRIEF HISTORY OF HEALTH PLANNING
- PART II PLANNING IN DIFFERENT RESOURCE ENVIRONMENTS
- 4 PLANNING IN THE CONTEXT OF RESOURCE ALLOCATION
- 5 PLANNING IN THE AUSTRALIAN PRIVATE HEALTH CARE SECTOR
- PART III CORE HEALTH PLANNING SKILLS
- 6 INFORMATION AND EVIDENCE FOR HEALTH PLANNING
- 7 IDENTIFYING HEALTH NEEDS AND ISSUES
- 8 COMMUNITY INVOLVEMENT IN HEALTH PLANNING
- 9 FORECASTING
- 10 DEVELOPING GOALS, OBJECTIVES AND STRATEGIES IN HEALTH PLANNING
- 11 SETTING PRIORITIES AND SELECTING INTERVENTIONS
- PART IV SPECIALIST HEALTH PLANNING PRACTICE
- 12 SERVICE PLANNING
- 13 PROGRAM PLANNING FOR HEALTH PROMOTION
- 14 CAPITAL PLANNING FOR HEALTH FACILITIES
- 15 CORPORATE AND BUSINESS PLANNING
- PART V IMPLEMENTATION ISSUES
- 16 ISSUES IN THE IMPLEMENTATION OF HEALTH PLANS
- 17 MONITORING AND EVALUATING HEALTH PLANS
- Bibliography
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Health Planning by Kathy Eagar,Vivian Lin,Pamela Garrett in PDF and/or ePUB format, as well as other popular books in Medicine & Health Care Delivery. We have over 1.5 million books available in our catalogue for you to explore.