![]()
Part 1
Control of Suffering
![]()
1
Pain Management at the End of Life
Clay M. Anderson
Pain is a universal aspect of life and part of our sensory experience. It is necessary and adaptive. At the same time, it is a form of suffering that can affect the duration and detract from the quality of human life. Currently, there are both pharmacologic and nonpharmacologic tools that allow us to modify pain in such a way as to minimize its impact on quality of life. This is a miracle of modern medicine. Still, around the world as well as in the United States, most pain sufferers are inadequately treated, for a variety of reasons.1 In other countries, the necessary medications may not be available.2 In the United States, the barriers to adequate pain modification include regulatory burdens, cost, myths about pain and pain medicines, and lack of education for the public and for medical professionals.3
Significant pain is present in the majority of patients dying of chronic diseases such as cancer, heart disease, lung disease, and diabetes.4 End-of-life care entails treating patients with these chronic diseases when the diseases are in their final phase, with the focus on bringing about relief of suffering and aggressively treating symptoms caused by the diseases. The common complaint of pain at the end of life is usually eminently treatable now, yet most patients remain undertreated.5 Here I will describe the problem of pain at the end of life and then show a way to optimally manage pain in this vulnerable population.
The Problem: Pain and Its Pathophysiology
Pain, one of many forms of suffering, is common at the end of life and is usually accompanied by a plethora of other symptoms, including dyspnea, nausea, confusion, anxiety, and depression.6 Pain seems to be the predominant symptom and also the most feared form of suffering.7 Pain at the end of life is protean and complicated. No two patients are alike in terms of the pathophysiology of their pain complaints or the psychosocial contexts of their pain. Pain at the end of life is undertreated, which is completely preventable. There is an ethical obligation in medicine and nursing to relieve suffering, and it is this directive that should lead physicians and other providers, as well as society in general, to bring down barriers and optimize pain management throughout life, but particularly at the end of life.
The pathophysiology of pain is complex, with new scientific discoveries in this area occurring frequently. I will now explain the basic concepts of pain pathophysiology so as to inform the rationale for optimal pain-management strategies. Nociception, the most upstream signal in pain physiology, occurs when tissue damage results in the stimulation of peripheral neuroreceptors in tissues, which, in turn, transmit a signal to a peripheral nerve. Transmission is the traversing of a pain signal from the nociceptor to the peripheral nerve to the spinal cord to the brain stem to the midbrain to the sensory cortex to the association cortex. Next is modulation, when, at least at the levels from the spinal cord and above, descending and local signals serve to either dampen or accentuate the ascending pain signals from the periphery. After modulation comes cognition, the final, summed subjective sensation of pain and modifying influences as experienced by the patient. Finally, expression is the communication of this cognition to others, verbally or nonverbally. Although simplistic, this schema allows us to get from a painful site in the body to the point where the person suffering the pain tells the provider about the pain in the context of his or her life and illness, and also shows us the levels at which any intervention might have an impact upon the pain.
Assessment and Therapy
Thorough assessment of pain is absolutely vital in order to treat it optimally and manage the disease causing it appropriately. This is true for diseases in the end-of-life phase as well as eminently curable conditions. Important factors in the assessment of pain include determining the following: location—subjective and anatomic description of where the pain is situated; chronicity—the duration of the pain complaint; temporal pattern—how the pain changes over time; severity—the intensity of the pain complaint, often measured from 0 to 10 (ordinal scale)8 or on a visual analog scale;9 character— how the pain is described, as sharp, dull, stabbing, burning, etc.; and associated findings—at the end of life, many other findings may be present, including dyspnea, cachexia, fever, depression, etc. A comprehensive approach to treating pain, one that takes into account both its characteristics and the results of the workup indicating possible etiology and/or a unique pathophysiology, is most likely to be successful.
Assessment, workup, and therapy sometimes occur nearly simultaneously in the real-life situation, but in general, an initial assessment and treatment is usually followed as soon as possible by a thorough workup in the outpatient or inpatient setting. The workup includes a physical examination—a good general examination with special attention to the neurologic and musculoskeletal findings; laboratory examination—judicious use of laboratory tests to confirm or refute suspected conditions causing the pain complaint (for example, infection or bone metastasis); radiographic evaluation—targeted radiographs including plain films, computed tomography, ultrasound, magnetic resonance imaging, and even positron-emission tomography; and other tests—for example, biopsies would be required to confirm a diagnosis of primary cancer or recurrence, and pulmonary-function tests or echocardiogram would address the severity of chronic obstructive pulmonary disease or congestive heart failure at a given point in time. This evaluation narrows the possible causes of pain, which are usually still numerous in dying patients, and allows for targeted therapeutics.
Therapy should occur simultaneously with the workup process, not upon completion of the workup. Either the outpatient or inpatient setting may be appropriate for evaluation and management of pain, depending upon the severity of the symptoms and the ease of control. The primary physician, nurse, psychosocial professional, and consultants should be involved as indicated from the beginning and should have the ability to communicate on a daily and preferably in-person basis. Through the workup and therapy, the target of the efforts should be the pain experienced and described by the patient.
Physicians and nurses both tend to focus heavily on the pharmacologic management of pain, but it is important to point out that there are multiple other therapeutic modalities that can impact pain in a positive way, and that the right mix of modalities for a successful therapeutic plan will be different for each patient. In addition to pharmacologic agents, other modalities include surgical intervention, other interventional techniques, palliative or radical radiotherapy, physiatry, massage, and electromagnetic therapy (for example, ultrasound or electrical stimulation).
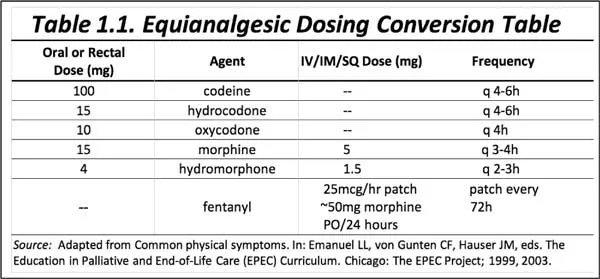
The principles of pharmacologic therapy for pain are well-established and have not changed dramatically in over three decades. Unfortunately, these principles are not being applied uniformly or effectively even in the United States. The World Health Organization formulated an analgesic-ladder concept in 1986 to serve as a guide to practitioners around the world regarding rational, effective use of non-opiate and opiate analgesics.10 Opiates are the mainstay of pharmacologic therapy for pain at the end of life because they are safe, effective, and easy to use from a pharmacologic point of view. There is no maximum dose of any pure opiate agonist. These medications have several drawbacks, including regulatory constraints, limited supplies (in some countries), and the real but uncommon problems of abuse, diversion, and addiction. Opiates come in weak, moderate, and strong agents; single-agent versus combination products; longacting versus short-acting formulations; and in forms for a variety of intended routes, including oral tablets/capsules, oral liquids, sublingual or transmucosal oral liquid or lozenge preparations, transdermal patches, suppositories, and solutions intended for the intravenous, subcutaneous, or intramuscular route. Most patients with chronic pain including at the end of life will do best with both a long-acting opiate formulation to prevent most pain and a short-acting opiate agent to treat episodic or breakthrough pain.11 It is relatively simple to choose an appropriate agent(s), dose, route, and schedule, and most of the time, with follow-up and adjustment as needed, this plan of treatment will be successful. If not, switching to another type of opiate often works. This is called opiate rotation, and it is successful about 50 percent of the time.12 In changing from one opiate agent to another, or from one route to another with the same or a different agent, an equianalgesic dosing table is quite helpful (see table 1.1).
In addition to opiates, other agents can have a direct or indirect effect on pain sensation or transmission. Traditionally, these other medications are called co-analgesics if they have analgesic properties on their own and adjuvant medications if they do not. The lines between these medications are becoming blurred as we learn more about their clinical and pharmacologic properties. Depending upon the type of pain—nociceptive, neuropathic, inflammatory, central, etc.—these other agents may add a great deal to what can be done with an opiate alone. In fact, on the WHO analgesic ladder, the first step is the use of acetaminophen or aspirin (or other nonsteroidal anti-inflammatory drugs [NSAIDs]) alone, without an opiate.13 These weak analgesics can control mild pain, even at the end of life, in many patients. Other categories of adjuvants or co-analgesic medications include anti-inflammatory agents (corticosteroids and NSAIDs), true adjuvants/neuromodulators (tricyclic antidepressants, anticonvulsants), psychiatric agents (antidepressants, anxiolytics, neuroleptics), and topical agents (lidocaine lotion or patches, capsaicin cream). Other medications are commonly utilized to minimize side effects from opiates and similar medications; these include stool softeners, laxatives, antiemetics, antacid medications, psychostimulants, and sedatives.
Adequate control of pain at the end of life requires aggressive application of multimodality therapy as needed. Of course, the most simple and straightforward plan of care possible would be the preferred one, yet many patients at the end of life truly require multiple complementary medications and other therapies. The plan should be as aggressive and multifaceted as is needed to achieve the goal of reasonable comfort or minimal suffering, along with maximal cognitive and physical function, in the context of the underlying disease process. Rapid, frequent reassessment is vital. Reassessment includes serial pain-scale measurements over time, repeat physician visits with physical exams, appropriate laboratory tests and radiographs, nurse reassessments, and analysis of home health and hospice evaluations. Each assessment should be followed by appropriate alterations to the plan of care, along with updated education of the patient and family caregiver. Changes in old symptoms or the appearance of new ones warrants more thorough investigations to look for treatable etiologies of the new symptoms. Methods of controlling the side effects of the opiates and other effective medications should also be reassessed along the way and changed accordingly.
Conclusion
The problem of undertreated pain at the end of life is still a major challenge for health-care providers. In the United States, all of the resources to solve this problem are at hand. For the vast majority of patients, the full and judicious use of these resources will result in a satisfactory to excellent outcome in terms of control of pain and related symptoms. In only a small percentage of patients will refractory symptoms remain or interventional procedures be required. Still, financial, regulatory, and attitudinal constraints remain as the main impediments to reducing the burden of pain at the end of life. Disseminating knowledge and effecting change in attitudes and policies must accompany the increased application of modern pharmacologic and nonpharmacologic therapies in a multidisciplinary setting. Although new agents are on the horizon, their absence should not be an impediment to success in this arena today.
Notes