- 320 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Reviews in Food and Nutrition Toxicity, Volume 4
About this book
Reviews in Food and Nutrition Toxicity, Volume 4 includes the most recent reviews of current issues involved in the toxicity of food and nutrients. With contributors from the fields of medicine, public health, and environmental science, the continuation of this series distills a broad range of research on food safety and food technology.
Vo
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicineSubtopic
Nutrition, Dietics & Bariatrics1 Heavy Metals in Breast Milk: Implications for Toxicity
Claudia Gundacker and Bettina Zödl
CONTENTS
Abstract
Abbreviations
Introduction
Sources of Heavy Metals and Transfer in the Environment
Exposure Routes and Biological Half-Life
Heavy Metals in Breast Milk
Exogenous and Endogenous Sources
The Process of Milk Production
Transfer of Heavy Metals into Milk
Mercury
Lead
Cadmium
Arsenic
Metal Concentrations in Breast Milk
Factors Influencing Milk Metal Contents
Mercury
Lead
Cadmium
Arsenic
Toxicological Implications
Mercury
Lead
Cadmium
Arsenic
Exposure Guidelines
Conclusions
References
Abstract Breast milk is unique as a matrix for biomonitoring, providing information about the metal body burden of women as well as the exposure of infants. The heavy metals mercury, lead, cadmium, and arsenic are widespread and persistent agents with significant dose-related toxicological implications at high exposure levels. However, the interrelationships under conditions of chronic exposure are not fully known. Metal in breast milk originates from exogenous sources, i.e., uptake via contaminated air, food, and drinking water, and endogenous release along with essential trace elements, which is characteristic for the reproductional period. Metal transfer into breast milk depends on the chemical form and the distribution of the metal in maternal blood fractions. Methylmercury is strongly bound to erythrocytes. A small quantity of methylmercury passes into breast milk and is easily absorbed by the suckling infant. Inorganic mercury is readily transferred into breast milk, but is not well absorbed by infants. Lead transfer is associated with casein. Human milk has a very low casein content; therefore, the excretion rate of lead is low. Because cadmium binds to metallothioneins, the mammary gland, like the placenta, is considered to serve as a barrier for cadmium and to protect the infant. Inorganic arsenic is not excreted in breast milk to any significant extent. The suckling infant may be exposed to toxic influences in a period of highest susceptibility. Metal toxicity is dependent on the chemical form involved, which determines the bioavailability, absorption rate, and retention time. The brain is regarded as the most important target organ of toxic impairment even at low doses. There is some epidemiological evidence that prenatal metal exposure (in particular, methylmercury exposure) correlates with neurodevelopmental deficits. Yet, it remains unclear whether and to what extent postnatal metal exposure through breastfeeding impairs the infant’s health. The toxicokinetics of arsenic among neonates and infants has been scarcely reported. As environmental and maternal conditions lead to significant differences in milk metal levels, all measures must be taken to avoid additional metal exposure of infants via breastfeeding.
Abbreviations As: arsenic; Ca: calcium; Cd: cadmium; Hg: mercury; K: potassium; Mg: magnesium; Na: sodium; Pb: lead; Po4: phosphate; Zn: zinc
INTRODUCTION
The American Academy of Pediatrics (AAP) firmly adheres to the position that breastfeeding ensures the best possible health as well as the best developmental and psychosocial outcomes for the infant. It is recommended that breastfeeding continue for at least 12 months, and thereafter for as long as mutually desired (AAP, 1997). There is no doubt that exclusive breastfeeding is ideal nutrition; yet it has to be considered that breast milk may contain pollutants, which implies the need to evaluate breast milk contents. Analyses of breast milk metal concentrations provide data about the metal burden in the woman’s body on the one hand, and metal exposure of neonates and infants via breastfeeding on the other. Therefore, breast milk is “unique as a matrix for biomonitoring, and analyses of breast milk for environmental chemicals as well as for nutrients are of wide scientific interest” (Needham and Wang, 2002).
Among diverse environmental pollutants, heavy metals belong to the most harmful xenobiotics, as they are widespread and persistent agents with significant doserelated toxicological implications. The persistence of metals, i.e., that they are not degradable, is one of their most problematic features and a major factor in the ecotoxicological relevance of heavy metals. The toxicology of metals is related to approximately 80 elements, including those heavy metals that, per definition, exceed a density of 5 g/cm3. Heavy metals of relevance in this context are mercury, lead, and cadmium. Arsenic is usually regarded as a hazardous heavy metal although it is actually a semimetal.
Humans are routinely exposed to environmental metal concentrations and accumulate metals accordingly, which results in a variety of health impacts. Heavy metals are known, or at least suspected, to possess an immunotoxic, mutagenic, carcinogenic, embryotoxic, and teratogenic potential. Their dose–effect relationships, however, are not fully known, especially under chronic exposure. Long-term, low-level metal exposure results in elevated metal burdens for the body. Such burdens are considered nontoxic as long as they are below health-based exposure guidelines; nonetheless they may impair human health.
Women of reproductive age are subject to a process known as body clearance, which may be defined as the loss of essential and nonessential elements during pregnancy and lactation due to the high nutrient demand at this stage. Lactating women (and subsequently their offspring) are affected by heavy metal exposure not only via exogenous sources, i.e., environmental exposure, but also through endogenous metal release. Hence the infant may be exposed to toxic influences in a period of highest susceptibility due to rapid growth, immaturity of kidneys and liver, and the unique vulnerability of the myelinizing central nervous system (CNS) to neurotoxic exposure. Furthermore, in cases of maternal element deficiency, the risk of toxic effects for both the infant and mother may be higher (Vahter et al., 2002); yet very few data are available on the interrelationships of essential and nonessential trace elements in breast milk.
Data on mercury, lead, cadmium, and arsenic transfer into and concentrations in breast milk are described in the following, as are the factors apparently responsible for increasing milk metal levels. Very few studies have been carried out on the distinct effects of metal exposure via breastfeeding, illustrating the difficulties in this concern: effects of postnatal exposure do not clearly separate from those of prenatal exposure.
SOURCES OF HEAVY METALS AND TRANSFER IN THE ENVIRONMENT
Heavy metals spread through natural and anthropogenic sources. Heavy metals are natural constituents of Earth’s crust, emitted by volcanic activity, forest fires, and rock weathering. Anthropogenic sources of heavy metals include various processing and manufacturing industries, mining, foundries and smelters, piping, waste disposal, and diffuse sources such as combustion of fossil fuels and by-products, constituents of products, and corrosion. Human activities throughout the last century have dramatically altered the biochemical and geochemical cycles of some heavy metals. Stumm and Keller (1984) presumed that, on a global scale, the anthropogenic emissions significantly exceed the natural emissions.
Once released into the environment, metals move between the atmosphere, land, and water. Physical properties determine whether an element is predominantly transported by the atmosphere or the lithosphere, which is particle-bound aquatic transport for the latter. Relatively volatile heavy metals and those that become attached to airborne particles can be widely dispersed on a very large scale.
The biosphere absorbs and accumulates various quantities of metals at certain trophic levels, depending on the environmental metal concentration, metal bioavailability, the feeding behavior, and the physiological state of organisms. In addition, some organic metal forms tend to accumulate along the food chain, e.g., methylated mercury. As a consequence, metallic elements are found in all living organisms and have potential toxicological implications for humans if the latter frequently consume species known to be accumulators of heavy metals, such as predatory fish, sea mammals, crustaceans, or shellfish.
EXPOSURE ROUTES AND BIOLOGICAL HALF-LIFE
The main exposure routes for humans are (1) inhalation of metal aerosols and metal vapor, (2) metal uptake through food and drinking water, (3) dermal metal absorption, and in case of the fetus, (4) uptake via the placenta.
After a metal has been taken into the lung or into the gastrointestinal tract, it will be deposited on the walls of the airways or will be taken up in the mucosa of the gastrointestinal tract, and a certain fraction of the deposited amount will be transferred to the systemic circulation and distributed among tissue compartments throughout the body (Camner et al., 1986). Several chemical and physical characteristics of metals in exposure media, such as air, water, and food, are important for absorption, excretion, and retention of metals by humans, and determine the specific biological half-life of metals.
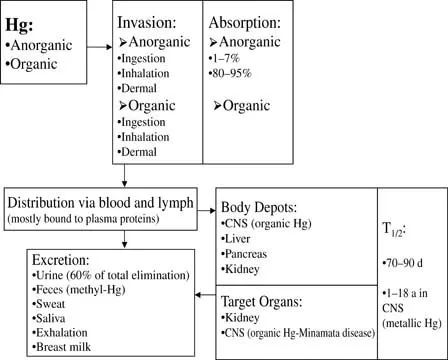
Mercury is readily absorbed (especially methylmercury in the gastrointestinal tract) and distributed throughout the body. Biological half-life varies from a few days to months; the organs with the longest retention times are the brain and kidneys (Figure 1.1). Vahter et al. (2000) presumed that the half-life of methylmercury is longer in fetal blood than in maternal blood, about 2 months in the latter.
About 10% of ingested lead is absorbed in the gastrointestinal tract. Infants and children may absorb as much as 50% of dietary lead. The main target organ of lead is the skeleton. The half-life varies among different tissue types. Lead retention in soft tissues is about 3 weeks, but in bone it may range from a few years to a few decades (Figure 1.2). Raghunath et al. (1997) reported retention times of 20 and 9 days for blood-lead and blood-cadmium in 6- to 10-year-old children, respectively. Gulson et al. (1999) described a longer lead half-life for infants than for mothers: 91 vs. 59 days.
Cadmium predominantly accumulates in the kidney. On account of its low excretion rate, cadmium has a very long half-life of 10 to 30 years in the muscle, kidney, and liver (Figure 1.3). Organic and inorganic arsenic have been shown to be readily absorbed via the gastrointestinal tract, and also by inhalation (Figure 1.4). Absorbed arsenic is widely distributed in the body; the highest levels are found in the hair, nails, and skin. The major part of arsenic in humans is eliminated within 10 days.
HEAVY METALS IN BREAST MILK
EXOGENOUS AND ENDOGENOU...
Table of contents
- Cover
- Half Title
- Title Page
- Copyright Page
- Preface
- Editors
- Contributors
- Table of Contents
- Chapter 1 Heavy Metals in Breast Milk: Implications for Toxicity
- Chapter 2 Selenium Toxicity and Its Adverse Health Effects
- Chapter 3 Arsenic in Fish: Implications for Human Toxicity
- Chapter 4 Biological and Toxicological Considerations of Dietary Sulfur
- Chapter 5 Fluoride – Toxic and Pathologic Aspects: Review of Current Literature on Some Aspects of Fluoride Toxicity
- Chapter 6 Bacterial Contamination of Ready-to-Eat Foods: Concern for Human Toxicity
- Chapter 7 T-2 Mycotoxin in the Diet and Its Effects on Tissues
- Chapter 8 Aflatoxin B1 and Cell Cycle Perturbation
- Chapter 9 Cycad Consumption and Neurological Disease
- Chapter 10 Dietary Lectins and the Immune Response
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Reviews in Food and Nutrition Toxicity, Volume 4 by Victor R. Preedy,Ronald Ross Watson in PDF and/or ePUB format, as well as other popular books in Medicine & Nutrition, Dietics & Bariatrics. We have over 1.5 million books available in our catalogue for you to explore.