The Progress in Infancy Research Series is dedicated to the presentation of innovative and exciting research on infants, both human and animal. Each volume in the series is designed to stand alone and contains autonomous chapters which are based on high quality programs of research with infants. These chapters integrate the work of the authors with that of other experts working in the same or related areas. The authors wish to present high quality critical syntheses bearing on infant perception and sensation, learning and memory processes, and other aspects of development. This series will be a forum for the presentation of technological breakthroughs, methodological advances, and new integrations that might create platforms for future programmatic work on the complexities of infant behavior and development.
Each volume in the series is dedicated to an outstanding investigator whose research has illuminated the nature of infant behavior and development, and whose contributions to the field have been of seminal importance.

- 328 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
Developmental PsychologyIndex
Psychology1
The Newborn as Informant
Lewis P. Lipsitt
Brown University
Brown University
The newborn’s psychobiological status is a product of congenital, prenatal, and birth conditions. Hereditary factors interact with intra-uterine biochemical factors, and both sets of conditions can be further complicated by obstetrical circumstances. By capitalizing on clinical–pediatric and behavioral assessment procedures, we should be able to carry out psychophysiological assessments on the newborn that will clearly reflect the course of and hazards inherent in embryonic and fetal development. Because specific prenatal hazards often have enduring effects, the newborn should be able to tell us whether things have gone badly or well. The neonate could become our collaborator in helping to forecast future developmental problems, and under the best of such circumstances might provide information about the probable success of various remedial interventions. The behavior of the newborn, in short, might provide the best, most valid indices of the “condition of the organism” that can be obtained. This dream is possible because so many advances have been made over the past two decades in the recording and understanding of sensory functioning, central nervous system integrity, and behavioral plasticity.
It is not too early for the behavioral scientist to apply already existing technologies for the benefit of infants born following a hazardous pregnancy. We should be better able to detect the character of the insufficiencies incurred and to plan the best possible remediation procedures for the problems discovered through close studies of sensory and learning processes in the young infant.
Many neonatal laboratories now use polygraphic recording procedures to document impairments due to prematurity, oxygen deprivation, and other perinatal conditions that tend to place infants in developmental jeopardy. Although it is well known that prematurity and anoxia contribute heavily to various developmental anomalies, including cerebral palsy, mental retardation, epilepsy, and school problems (Drillien, 1964; Sameroff & Chandler, 1975), much research remains to be done to develop the best clues for the early detection and amelioration of these conditions (Gluck, 1974; Lipsitt, 1977).
This chapter reviews several areas of behavioral investigation of the newborn, with emphasis on those procedures that have shown special promise for the eventual better detection of neonatal aberrations and their sequelae. The promising techniques to be considered are those that have yielded interesting and stable individual-difference data in groups of normal infants and provided some preliminary findings suggesting that they may have special use in detecting early deficits related to later cognitive functioning. The propositions to be considered are:
- Careful measurement of sucking behavior in the normal newborn, when appropriated for use with premature, small for dates, and otherwise stressed infants can have special value, particularly if questions are asked about patterns of response, rather than merely about whether the infant has a particular response in its repertoire. It should be more illuminating to ask not only whether the infant can hear or suck, but also whether the psychophysical curve relating the baby’s response to various stimulus intensities matches that for other infants of the same age. We thus not only ask whether the infant detects a new taste, but also whether its adaptation to the new taste resembles that of normal infants who show an orderly accommodation of responses to different concentrations of sweet fluid.
- The detection of sensory and behavioral deficit will probably be facilitated by the intensive study of habituation, which capitalizes upon the organism’s accommodation to external stimuli. The infants are asked not only to detect a light of moderate intensity, but to report on changes in their defensive or orienting “attitude” toward repetitive presentations of the same stimulus. The inability of infants to show psychophysiological change to such redundant stimulation has been shown in preliminary studies to be a mark of nervous-system (probably cortical) immaturity or central nervous system (CNS) damage.
- Stimulation of premature infants with special procedures for providing extra experience has suggested that infants who may be predicted on an actuarial basis to be retarded or to show some deficit later in life might benefit from compensatory stimulation. Such extra input, in anticipation of the predicted deficit, could succeed in mitigating the loss.
- There are presently some indications that the so-called “sudden infant death syndrome” (crib death) is a disorder of development that might have some anticipatory components detectable during the earliest days of life. The early leads into an understanding of this matter require much additional work, because we cannot know the possibilities until the plausible existing hypotheses have been pursued. The supposition is put forward here that at least some crib deaths, which occur mostly between 2 and 4 months of age, may be due to a failure to undergo critical experiences during the first 2 months of life. By the age of 2 to 4 months, many responses that were initially unconditioned or obligatory become executed on an operant or more “voluntary” basis. During the early months, the infant must learn to engage in “respiratory retrieval responses” in order to respond properly to potentially lethal threats of respiratory occlusion.
POLYGRAPHIC STUDIES OF THE NEWBORN’S SUCKING AND HEART RATE
Recent advances in the use of polygraphic recording in infant research, and the exquisite sensitivity and responsivity of the newborn to exteroceptive stimulation, have led to considerable progress in our understanding of the sensory and learning capabilities of the newborn. The developmental psychologist’s capability for conducting refined assessments of the neonate’s sensorium has brought us closer to doing informative longitudinal studies, both short- and long-term. These investigations are necessary not only to discover whether certain very early experiences may have a lasting effect upon the behavior and well being of the baby, but also to find whether stimulus interventions may have salubrious consequences for a child who might otherwise manifest a later developmental deficit. It is not too early for us to hope that it might be possible to provide immunity, through behavioral techniques, against some sorts of developmental anomalies. First, however, it is necessary to seek solid documentation of the sensory capacities and behavioral repertoire of the very young infant (Lipsitt, 1977).
In this spirit, a number of studies have been carried out in my laboratory at Women and Infants Hospital of Rhode Island to find out, for example, about the neonate’s capacity for discriminating odors and tastes. Through both of these senses the newborn relates closely with the world in the first hours following birth. Our studies have generated some data relating to the approach and avoidance style of the newborn, the differ- ences among newborns in such styles, and the reactions of babies to stimuli that adults would regard as pleasant and unpleasant. In this section, several studies are reviewed from which the inexorable conclusion is drawn that the baby is keenly sensitive in the first few hours of life to subtle changes in gustatory stimulation.
The baby acts on its discrimination of these taste changes either to promote the perpetuation of the taste or to suppress it, depending largely upon sweetness. In short, the newborn is a hedonic creature who responds to the incentive-motivational properties of reinforcers with both motor changes in behavior, such as in sucking and swallowing, and autonomic behavioral changes. The autonomic aspects of these behavioral consequences of pleasant and unpleasant stimulation, such as the accompanying heart-rate changes, are, of course, the rudiments of affect. There is no mistaking the most avid manifestations of such affect, as when the infant goes quickly quiet when offered a sweet fluid. Mothers do indeed respond sympathetically and reciprocally to these behaviors in their newborns by, for example, moving to promote the baby’s search for the nipple and the sweet taste or by helping the baby to escape momentary respiratory occlusion when awkwardly positioned. Mothers and fathers usually respond quickly with looking, touching, and lifting when the baby cries; this is, in fact, a good example of the infant and its caretakers “pleasuring” each other.
Our studies of neonatal taste are carried out in a special crib, housed in a white, sound-attentuated chamber with temperature about 80˚ Fahrenheit. Ambient light is about 50 foot-candles. Breathing is monitored by a Phipps and Bird infant pneumobelt around the abdomen and respiration and body activity recorded continuously on a Grass polygraph. Hewlett- Packard electrodes are placed on the chest and leg, permitting polygraphic monitoring of the primary heart rate, which is then integrated by a Hewlett- Packard cardiotachometer and recorded on another channel.
Sucking is recorded on one of the polygraph channels, using a “suckometer,” which consists of a stainless-steel housing with a pressure transducer, over which a commercial nipple is pulled. A polyethylene tube runs into the nipple from a pump source and delivers fluid under the experimenter’s control and, in most of our studies, on demand of the subject. When delivering, the pump ejects into the nipple-end a tiny drop of fluid contingent upon the execution of a sucking response of preset amplitude. The size of this drop for each criterion suck is usually 0.02 ml although in some studies in which the effect of the magnitude of the drop is under study, the drop amount may be varied from 0.01 ml to 0.04 ml. See Figs. 1.1 and 1.2.
The situation is arranged such that the infant may receive no fluid for sucking, or might receive a fluid such as sucrose or dextrose in any desired concentration. Contingent upon sucking, one drop of fluid is ejected into the baby’s mouth for each suck. A polygraph event marker records fluid ejections during fluid delivery periods or the occurrence of a criterion suck during no-fluid conditions. A 74 dB background white noise assures a fairly constant acoustical environment in the infant chamber.
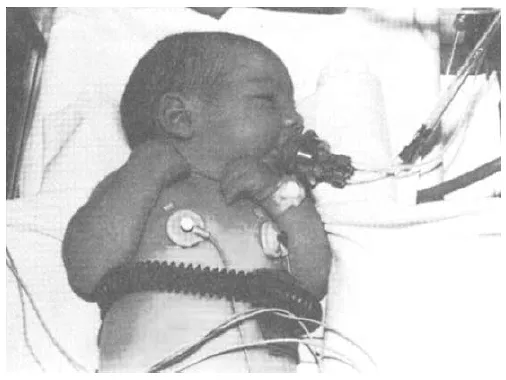
FIG. 1.1 Two-day-old infant prepared for recording of respiration, heart rate, and sucking.
The laboratory nurse initially makes contact with the mother to explain the research program and obtain informed consent. When the infant is brought to the laboratory for testing, the electrodes and pneumobelt are applied and the infant is swaddled and placed on its left side. The nipple is inserted, supported by a cushion to enable recording without touching the baby. During the first few sucking bursts on the nipple, no fluid is delivered, and the experimenter calibrates the equipment. Preamplifier sensitivity is adjusted for each infant so that the average sucking amplitude results in a 5 cm excursion of the polygraph pen. The threshold criterion is then set at half this excursion, and only those responses exceeding that minimum are considered as criterion responses.
Newborns characteristically suck in bursts of responses separated by rests. Burst length and rest length both constitute individual-difference variables under no-fluid conditions, i.e., some newborns engage in reliably longer bursts and pauses than others. Both of these parameters, as well as the sucking rate within bursts, however, are significantly influenced by the conditions that are prearranged as the consequences of an infant’s behavior. With a change from a no-fluid condition to a fluid-sucking condition or from sucking for a less-sweet solution to a sweeter solution, several behavioral consequences characteristically occur. There is a tendency for the sucking bursts to become longer, for the inter-burst intervals to become shorter, and for the inter-suck intervals to become longer. Thus, sucking rate within bursts becomes slower with increasing sweetness of the fluid, and the infant takes fewer and shorter rest periods.
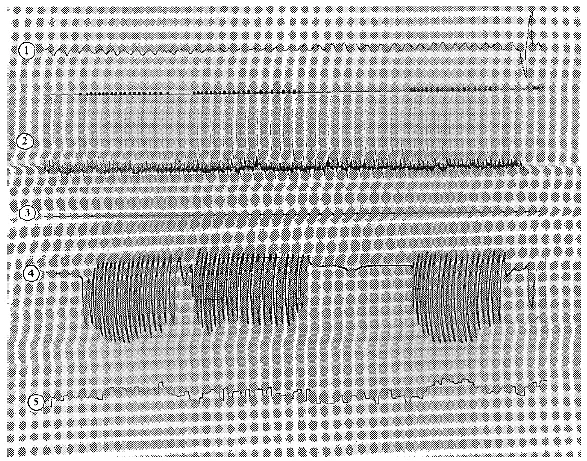
FIG. 1.2. Polygraph recording of (1) respiration, (2) electrocardiogram, (3) blank channel, (4) sucking, and (5) electrocardiotachometer, with digital representation between channels 1 and 2 of the sucking responses recording in channel 4.
Contrast Effects
The aforementioned regularities of response in relation to the incentivereinforcement conditions imposed upon the infants during polygraphic testing make it possible (a) to explore the effects of a previous taste experience upon the infant’s response during a subsequent taste experience and (b) to investigate the interrelationships of these various suckingresponse parameters and their relationship to certain other response measures, such as heart rate. Kobre and Lipsitt (1972) tested infants for 2 minutes on the nipple without any fluid delivery whatever. Subjects in this study were rejected for further study if they had a mean sucking rate lower than 30 per minute during the 2 minute period. The 25 subjects remaining were divided into five groups. A total of 20 minutes of responding was recorded for each subject in four successive 5-minute periods. Between each period the nipple was removed for 1 minute to allow the tube to be flushed with water and the child to be picked up.
These 25 infants, most 3 days old, received one of five reinforcement regimens for the 20-minute period. One group received only sucrose. A second group received water throughout, and a third received sucrose and water, alternated twice, in 5-minute units. A fourth group received no fluid throughout the four 5-minute periods and was compared with a group that received sucrose alternated with no fluid in 5-minute periods.
Frequency polygons of the inter-response times, or inter-suck intervals, were printed out on the console of an on-line PDP-8 computer. Comparison of the first three groups revealed that sucking rate within bursts slows down for a fluid-sucking condition relative to no-fluid sucking and that sucking rate becomes still slower for sweet-fluid sucking relative to sucking for plain distilled water. Thus, there is an orderly progression from no fluid to plain water to 15% sucrose sucking, with sucking response becoming slower and slower as the incentive value of the reinforcement delivered consequent upon the response increases. Also, under the sucrose condition, the infants invested a larger number of responses during a comparable period of time than under either the water or no-fluid condition. This effect, which was a consequence of the infant taking fewer rest periods under the higher incentive condition, also occurred in the comparison of responses emitted for water compared with no fluid.
In this study, the infants who sucked for sucrose throughout the 20-minute testing period emitted significantly more responses per minute than did the group that received water throughout the 20-minute period. Moreover, both groups showed stable response rates for their respective fluids through the four blocks of 5 minutes each. The most interesting finding in this experiment, however, concerned subjects who were alternated from one 5-minute period to another between sucrose and water, or between sucrose and no fluid. These groups showed marked effects attributable to the alternating experiences. For example, when sucking for sucrose, the sucrose/water group was essentially comparable to the group sucking for sucrose throughout. When switched to water, however, response rate during each of those 5-minute periods was significantly lower than in their counterpart controls in the water-throughout group. Thus, when newborns have experience in sucking for sucrose, an immediately subsequent experience with water “turns them off.” They display their apparent “aversion” for the water by a marked reduction in instrumental behavior that would put that fluid in their mouths. When the consequence of the re- sponse is changed, as from water to sucrose, response rate goes back to a normal level. The infant thus optimizes taste-incentive experiences by modulating oral behaviors pertinent to their occurrence.
The same type of effect occurred in the sucrose/no-fluid group, which showed lower response rates when sucking for no fluid after experience in sucking for sucrose. These negative contrast effects were reliable, and there is no reason to suppose that the phenomenon is not widespread throughout the range of incentive conditions to which neonates would be normally subjected. We would expect such effects to occur whenever the infant is called upon to “compare and contrast” two levels of incentive, such as formula vs. plain water or breast-milk vs. a sweeter formula.
Newborns, then, seem strikingly affected in their subsequent behavior by experiences within the immediately previous 5 minutes. The negative contrast effect demonstrated here is one of the most rudimentary types of behavioral alteration due to experiential circumstances. As with neonatal habituation to olfactory stimulation (Engen & Lipsitt, 1965), the suggestion is that memorial processes are already working in the newborn, such that there is a lasting impression made, admittedly of unknown duration, of the experience endured. These are the beginnings of learning processes.
Relations Between Sucking Behavior and Heart Rate
We now know that at least some aspects of the motor behavior of the newborn are modulated to accord with the incentive conditions to which the baby is exposed. Several studies have reinforced this impression and have further provided us with data on the rudiments of affect in the neonate in the form of changes in autonomic responding depending on incentive conditions.
A study of 44 normal full-term newborns, 24 males and 20 females, was conducted on two consecutive days using the same polygraphic techniques (Lipsitt, Reilly, Butcher, & Greenwood, 1976). On the first day of testing, the mean age of the infants was 54 hours and, on the second day, 78 hours. Eleven of the infants were breast-fed and the remainder bottle-fed.
Immediately following calibration of the apparatus, a period of 10 minutes of sucking was recorded for each infant in five successive periods, each of 2 minutes duration. Three of these periods were spent sucking for no fluid, followed by two periods of 15% sucrose-sucking. About 35 seconds intervened between periods, during which time a computer printed out the inter-response time data (IRT) for the preceding period. The nipple was not removed between periods, and the infant continued sucking under the same condition as in the preceding period. The beginning of a period, following the 35-second print-out, was initiated after the infant stopped sucking for at least 2 seconds and after the end of a burst. Following the second sucrose period, the nipple was removed. A 2-minute period of polygraph recording then ensued during a “resting” state, defined as quiescent and with regular respiration, in which the infant neither sucked nor was stimulated in any way.
The results suggest a very interesting interplay between the sucking response and heart rate. They further substantiate a process supporting our supposition that a “savoring mechanism” seems to be operative in the earliest days or even minutes of life.
The computer print-out at the end of each 2-minute period provided a frequency distribution of sucking IRTs in 100 msec bins for inter-suck intervals under 2 seconds. The mean IRT could be calculated from the printout, using the midpoint of the bin as its numerical representation.
The sucking data from this study essentially replicated those of the previously reported study in showing that under no-fluid sucking, significantly more rest periods (defined as IRTs greater than 2 seconds) were engaged in than for 15% sucrose sucking, fewer responses per burst occurred for no-fluid sucking, and both the modal and mean IRT for no-fluid sucking were reliably shorter than for sucrose sucking. In addition, more responses per minute were emitted for sucrose than under the no-fluid condition.
A feature of the data that was rather a surprise was the seemingly paradoxical increase in heart rates during sucrose-sucking conditions where the sucking rate within bursts was slower. This effect, like all of the suckingparameter effects, occurred on both the first and second days of the study. During basal recording, the heart-rate mean was approximately 116 beats per minute. When sucking for no fluid, the rate rose to 124, and when sucking for sucrose the rate rose further to 147. Thus, although sucking rate within burst was reduced when the in...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- List of Contributors
- Preface
- Dedication
- Reminiscence and Rumination
- 1: The Newborn as Informant
- 2: Memory for Hidden Objects in Early Infancy: Behavior, Theory, and Neural Network Simulation
- 3: Connectionist Methods in Infancy Research
- 4: Flexibility and Specificity in Infant Motor Skill Acquisition
- 5: Limitations on Visual Sensitivity During Infancy: Contrast Sensitivity, Vernier Acuity, and Orientation Processing
- 6: A Model of the Origins of Autobiographical Memory
- 7: Categorization of Infant-Directed Speech
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Progress in infancy Research by Jeffrey W. Fagen,Harlene Hayne in PDF and/or ePUB format, as well as other popular books in Psychology & Developmental Psychology. We have over 1.5 million books available in our catalogue for you to explore.