eBook - ePub
Nutrition and Heart Disease
Causation and Prevention
- 360 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Nutrition and Heart Disease
Causation and Prevention
About this book
Heart disease is the primary cause of death and disability in Western countries. Research indicates that nutrition and diet play key roles in both preventing and causing many types of heart damage and dysfunction. By understanding the complex relationship between diet and disease, new prevention measures can be established and millions of lives can
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Section III
Foods and Macronutrients in Heart Disease
10 Flavonoids Extracted and in Foods: Role in Hypertension Prevention and Treatment
Cynthia Mlakar, Katrina Simpson, and Ronald R. Watson*
10.1 INTRODUCTION
This chapter addresses the possible role of flavonoids in the prevention and treatment of hypertension. It begins with a concise description and the probable causes of hypertension. Comorbidity rates, as well as the resultant widespread financial impacts on the health system associated with hypertension, are mentioned. Current medical antihypertensive treatments are briefly summarized, along with the side effects considered partially responsible for patient noncompliance with therapies. Dietary suggestions and alternative herbal remedies are reviewed, leading into a discussion of flavonoids — plant substances gaining popularity for their prevention and remedial effects on a variety of diseases and ailments. Studies of the blood pressure lowering effects of flavonoid ingestion are cited.
Hypertension, also known as high blood pressure, is the most common reason for patient visits to primary care offices.1 One study showed that up to 70% of all doctor visits in 1995 were concerned with hypertension.2 In 1998, 50 million people in the U.S. were diagnosed with hypertension.3 Hypertension is at the top of the lists of many health care systems1 and is one of the costliest and most complex diseases to treat. In 1995, $18.7 billion was spent in the U.S. to treat hypertension.2,4 Approximately 20% of that amount was spent on drug treatment.2 The costs of treating high blood pressure represent large and increasing proportions of health care costs in many countries.4 The higher rates of hypertension noted in formerly communist countries were originally presumed to result from the increased consumption of cereals and more obesity.5 However, the incidence of hypertension is probably influenced more by the lack of fresh fruits and vegetables in winter and spring and the high levels of alcoholism, smoking, and pollution that enhance production of free radicals.5
The high cost of treating hypertension is a result of the complexity of the disease. Often referred to as a “silent killer,” hypertension has a high degree of comorbidity. In other words, hypertension causes or is connected with many other diseases. This fact makes hypertension more complex to manage because several providers of different types of care may be involved in various treatments, and multiple mechanisms may be required to manage high blood pressure.4 The inflammatory reaction of chronic venous insufficiency (CVI) may be triggered by venous hypertension.6 Additionally, hypertension is chronically present over a long period of time in a patient’s life.1
Hypertension is a significant cause of major organ damage, usually as a result of inadequate treatment.7 Because it is asymptomatic and produces few or no tangible effects, patients often ignore advice and fail to comply with treatments prescribed for this chronic disease. Hypertension is the most prevalent risk factor for atherosclerosis, which affects approximately 43 million persons in the U.S.8 Strokes, heart attacks, and other cardiovascular diseases can also be caused by hypertension.9 Studies indicate hypertension predisposes those who have it to all major atherosclerotic diseases,4 and researchers cite hypertension as one of the three most preventable causes of cardiovascular mortality.5 Other sources argue that the risk of heart disease in hypertensive populations is the same as the risk for nonhypertensive populations.10
Some studies indicate that only 47% of patients with hypertension achieve optimal blood pressure control (measurements below 140/90 mmHg).8 Tight blood pressure control is considered more effective than glycemic control in preventing macrovascular events.11 A strong association exists between high blood pressure and intermittent claudication and other symptoms of peripheral arterial disease (PAD). Type I diabetes mellitus is associated with peripheral macrovascular and microvascular disease.8
High blood pressure is defined as an excessive amount of energy generated by the force of blood flowing against the walls of arteries.12 Over 80% of patients with high blood pressure fall within the borderline to moderate range;13 that is, they have systolic blood pressures of 120 to 180 mmHg and diastolic blood pressures of 90 to 114 mmHg. High blood pressure is often considered a systolic pressure above 140 and a diastolic pressure above 90 mmHg.13
10.2 TYPES AND CAUSES OF HYPERTENSION
Essential or primary hypertension is defined as a medical condition denoted by consecutive high (above 140/90 mmHg) blood pressure readings in the absence of a known causal disease.14 It is the result of elevated arterial pressure associated with increased cardiac output, total peripheral resistance, or both.15 Unfortunately, mystery exists about the causes and treatment of this form, even though 95% of all hypertensive patients have essential hypertension.9 Primary hypertension affects approximately one-third of the world’s adult population.4
Secondary hypertension is the sudden onset of high blood pressure in children or people over the age of 50.9 A mere 5% of those with hypertension have the secondary type.9 Systemic arterial hypertension is one of the most common cardiovascular diseases of industrialized populations. It affects approximately 20% of adults in these societies, and the percentage is higher among the elderly and blacks.15 Males were at higher risk to develop hypertension, but greater risks for women have been noted in the past decade.16 Malignant hypertension is the most severe form. It progresses rapidly and proves fatal within 5 years for 90% of its patients.9
Essential hypertension can result from narrowed arteries, from circulation of a greater-than-normal volume of blood through the body, or a combination of both factors.12 Arteriosclerosis is a narrowing of the smaller arteries recognized as a major pathophysiological change in essential hypertension.17 In order to function well, arteries must have elasticity. Serotonin occurs naturally in the body and is believed responsible for causing constriction of the large arteries while causing arterioles and large veins to vasodilate.18
The sympathetic nervous system or insulin resistance can also cause hypertension.19 Abnormal renin that triggers angiotensin21 and oxidation that produces aldosterone21 are further risk factors.19 Other causes of clinical variable hypertension are physiologic variables.22 The first is vascular tone, which establishes the elastic properties of veins and arteries, vessel diameter, and vascular resistance.22 Additional variables causing high blood pressure are inotropic state and heart rate.22 Hypertension can result also from the use of drugs, medications, and other substances such as oral contraceptives, nonsteroidal anti-inflammatory drugs, licorice, cocaine, and amphetamines.23
Obesity and diet factors are other issues considered as causes for hypertension because 50% of obese people have hypertension.9 Possible dietary causes for hypertension include high intake of salt and fats.24 Processed foods and many snack foods are high in sodium content. Although modern society embraces the fast food concept, fast foods may not be as healthy as we want or need. Actions to promote awareness of the risks associated with this type of daily dietary intake have met with resistance. “The possible loss of income to the salt and soft-drink industries that might follow moderate sodium reduction has led to the formation of lobbying operations in several countries that work against efforts to reduce sodium intake.”25
An elevated level of dietary salt (NaCl) is thought to be a cause of hypertension. By the late 1940s, the role of dietary salt as a cause of hypertension had been studied and debated for over 100 years.26 “The prevalence of hypertension and its consequences is [sic] linearly linked to dietary salt intake in societies throughout the world.”27
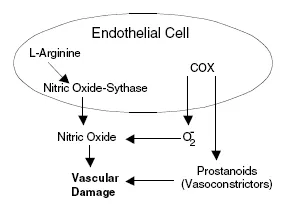
FIGURE 10.1 Vascular damage caused by functions within the endothelial cell.
Endothelial cells are important mediators of vasoconstriction and vasodilatation. This mediation is brought about by the production of nitric oxide (a vasodilator) by the endothelium.28,29 Inhibition of platelet aggregation relaxation are some ways nitric oxide can affect the body.30 Alterations in L-arginine, a compound that forms nitric oxide, can lead to a decrease in nitric oxide production and high blood pressure. While not directly related to nitric oxide, cyclooxygenase (COX) can cause vascular damage by producing superoxide anions and prostanions31 (see Figure 10.1).
10.3 CURRENT MEDICAL TREATMENTS FOR HYPERTENSION
Hypertensive drugs are normally taken on a continuous basis.9 In diseases such as hypertension, diabetes, and asthma, a relapse following cessation of treatment is considered evidence of the effectiveness of the treatment and the need to continue monitoring the patient.32 The six main drug treatments for hypertension are diuretics, beta-blockers, calcium antagonists, angiotensin-converting enzyme (ACE) inhibitors, angiotensin II antagonists, and alpha-adrenergic blockers, although no reliable data support the last two regimens.23
Beta-blockers interfere with the absorption of epinephrine, leading to decreases of heart rate and blood pressure, although caffeine, alcohol, and salt can reverse the effects.8 Furthermore, an increase of triglycerides may result from the use of beta-blockers.33,34 Diuretics may impair lipid profile, cause glucose intolerance, and result in elevation of uric acid.33 Resperpine and methyldopa are also used in some parts of the world. Aspirin is used as an antiplatelet therapy.23
Possible new drugs are constantly on trial, for instance, vasopeptidase inhibitors.9 Sildenafil specializes in pulmonary vasodilation; while it increases blood flow out of the heart, it has no effect on wedge pressure.35 One group of researchers attempted to determine whether benazepril or nitrendipine produced a “greater reduction in left ventricular mass.” The results were close: benazepril had greater effect on diastolic pressure and nitrendipine decreased systolic pressure more.32
Keeping in mind the terrible risks the disease involves, some people with high blood pressure do not feel any warning signs and thus fail to realize they have a major illness.9 They feel fine and the treatments are expensive and...
Table of contents
- Cover Page
- Title Page
- Copyright Page
- Preface
- Editors
- Contributors
- Section I
- Section II
- Section III
- Section IV
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Nutrition and Heart Disease by Ronald Ross Watson, Victor R. Preedy, Ronald Ross Watson,Victor R. Preedy in PDF and/or ePUB format, as well as other popular books in Medicine & Cardiology. We have over 1.5 million books available in our catalogue for you to explore.