- 158 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Disorders of the Cervical Spine
About this book
Disorders of the Cervical Spine focuses on the various problems of the cervical spine. This book discusses how disorders of the cervical spine affect the vital structures and movement of the head relative to the neck and the neck relative to the head. Organized into 10 chapters, this book begins with an overview of the structural anatomy of the neck. This text then examines the contributions of radiology to the management of patients with injury or disease of the cervical spine. Other chapters consider the congenital deformities and anomalies of the cervical spine. This book discusses as well the common injuries as well as the more unusual injuries of the cervical spine. The final chapter deals with the episode of the operation in the management of cervical injury or disease, which is preceded by meticulous clinical and radiological assessment of the patient. This book is a valuable resource for orthopedic surgeons, neurologists, neurosurgeons, rheumatologists, radiologists, and general physicians.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicinaSubtopic
Enfermedades y alergias1
Applied anatomy
Publisher Summary
This chapter discusses the important structures of the neck, most of which can be seen and felt in the thin patient. Few of these structures are apparent in the obese, pyknic individual with a short neck; however, certain landmarks can always be found. The sternomastoid muscle, running from one corner to the other of a quadrilateral area, formed by the anterior midline, the clavicle, the leading edge of the trapezius, and the mastoid–mandibular line divides the side of the neck into anterior and posterior triangles. The apophyseal joints lie oblique in the sagittal plane and incline medially in the coronal. This alignment lacks the architectural stability of the dorsal and lumbar areas of the spine; however, it permits more movement. A fail-safe locking mechanism is provided by the abutment of the superior leading edge of the inferior facet into the articulo-transverse angle of the joint above. The joint capsules are richly innervated with pain and propioceptive receptors—more so than in the corresponding joints lower in the spine—so that awareness of head and neck movement is enhanced.
‘Was common clay ta’en from the common earth Moulded by God, and tempered with the tears Of angels to the perfect shape of man.’
‘To–’, Tennyson, 1851.
INTRODUCTION
Man sees before he understands. The accuracy (but not the beauty) of Leonardo da Vinci’s anatomical drawings, astonishing and unsurpassed after 400 years, disappears in his portrayal of structure whose function was not known to him. He knew what bones and muscles do, and could interpret their anatomy in architectural and engineering terms; and he drew them with a photographic regard for correct detail. He was the first biomechanic. He did not know what nerves do, and drew them as he thought they should look according to the metaphysics of Galen and Bacon∗. We can not afford to smile at their naivety. We are as guilty of false extrapolation, and as restricted by orthodoxy as the medieval philosophers. Vesalius was four years old when Leonardo died. Within one generation the foundations of topographical anatomy, derived from dissection, had been laid so securely that all further details of anatomical knowledge have been mere additions to Vesalius’ work.
This is not the place to discuss the importance of descriptive anatomy in the undergraduate curriculum; but its position in the clinician’s approach to accurate diagnosis and management remains paramount and unchallenged. In recent years much attention has been paid to the detailed topographical structure of the neck. This chapter is unashamedly selective in concentrating on some of these aspects. It is not an attempt to teach anatomy to the orthopaedic surgeon; or to replace the cadaver and Gray as his primary source (even less is the word ‘primary’ a Freudian slip).
The neck conveys vital structures from and to the head and trunk. It enables the head to be placed in a position to receive from the environment all information other than that provided by touch. We need to know as much as possible about these structures, about movement of the head relative to the neck and the neck relative to the trunk; disorders of the cervical spine will affect one or other of these things.
SURFACE ANATOMY
Many of the important structures of the neck can be seen and felt in the thin patient. Less is apparent in the obese, pyknic individual with a short neck, but certain landmarks can always be found.
The sternomastoid muscle, running from one corner to the other of a quadrilateral area, formed by the anterior midline, the clavicle, the leading edge of the trapezius and the mastoid–mandibular line, divides the side of the neck into anterior and posterior triangles (Figure 1.1).
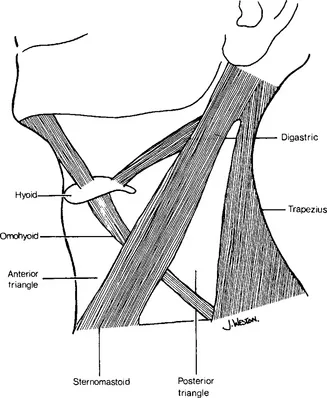
Figure 1.1 Muscular triangles of the neck
The posterior triangle contains little which is visible on inspection. Palpation of the base of the triangle (which is really a pyramid) finds the first rib, crossed by the subclavian artery, the lower trunks of the brachial plexus and perhaps a cervical rib or its fibrous prolongation. Higher, the accessory nerve, running forwards to the sternomastoid, divides the triangle into an upper ‘safe’, and a lower ‘dangerous’ area (Grant, 1951). In this upper area the transverse processes of the cervical vertebrae can be deeply felt.
There is more to be seen, and felt, in the anterior triangle. The external jugular vein, and the platysma, cross the sternomastoid; and both stand out in the thin singer. The ‘Adams’ apple’∗ moves with swallowing, and the pulsation of the carotids is often visible. Below the body of the hyoid, the neurovascular bundle can be compressed against the carotid tubercle of the sixth vertebra; demonstrating how easily accessible is the spine through this area. In the apex of the triangle, the transverse process of the atlas is palpable immediately behind the internal carotid artery; and the finger tip can roll over the tip of the styloid process and the stylohyoid ligament. In the anterior midline can be usually seen, and always felt, the anterior arch of the hyoid, the notch of the thyroid cartilage, the cricoid and the upper rings of the trachea. With advancing age, the horizontal creases in the skin become more pronounced. Whenever possible, operative incisions should occupy one of these creases, in the interests of healing, if not beauty.
The currently fashionable long hair of both sexes makes inspection of the back of the neck difficult. Fortunately, fashion is fickle. The vertebra prominens, which may be the spinous process of the seventh cervical or the first thoracic vertebra, marks the lower end of the midline sulcus formed by the ligamentum nuchae in its leap to the occiput. The rounded ridge on either side of the sulcus is made by splenius capitis as the origin of trapezius is tendinous. The vertebra prominens is the top of the ‘dowager hump’ seen in patients with cervical spondylosis.
THE CERVICAL VERTEBRAE
The atlas
The atlas has no body (Figure 1.2). The anterior arch is faceted to receive the tip of the odontoid process, and the medial aspect of each articular mass is indented by the attachment of the transverse band of the cruciate ligament. The spinal canal at this level is spacious. Its sagittal diameter may be divided into three; the anterior third being occupied by the arch of the atlas and the odontoid peg; the middle third by the cord; and the posterior third by the subarachnoid space. Cisternal puncture by the posterior or lateral route is therefore safe under normal conditions.
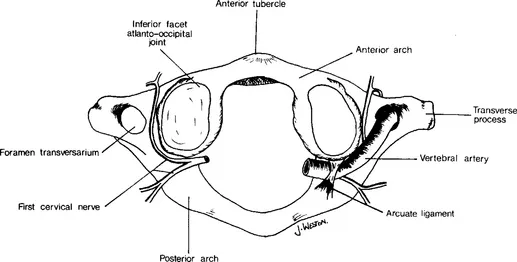
Figure 1.2 Atlas, superior aspect
The oblique groove across the posterior arch of the atlas accommodates the vertebral artery after it has wound around the outside of the articular mass. The attachment of the posterior atlanto-occipital membrane is arched over the artery at this point, and this arch is sometimes outlined, completely or incompletely, by bone to form the arcuate foramen. The significance of this bony arch is commonly regarded as negligible; but it has been said that its presence renders the atheromatous vertebral artery more vulnerable to compression during rotation of the head (Klausberger and Samec, 1975).
The side-to-side width of the atlas is greater than that of any other cervical vertebra, to increase the leverage of the muscles inserted into the transverse process. This transverse process is the only one in the cervical spine which is not grooved to allow egress of a nerve root. The articular masses are broader and deeper than any other because they shoulder the weight of the skull, and also because the inferior articular facets lie directly below the superior, not behind them as do the inferior facets of the subjacent apophyseal joints.
The axis
The axis has stolen the body of the atlas (Figure 1.3) to form the odontoid peg which projects up from its centrum to lie behind the arch of the atlas. The tip of the odontoid is faceted in front to mate with its atlantic fellow, and behind to accommodate the synovial bursa which separates it from the transverse band of the cruciate ligament. On either side of the base of the odontoid, the centrum presents the inferior facets of the atlanto-axial joints. Below, the atlas begins to take on the characteristics of a typical cervical vertebra. Its laminae meet to project a bifid and massiv...
Table of contents
- Cover image
- Title page
- Table of Contents
- Dedication
- Copyright
- Inside Front Cover
- Foreword
- Preface
- Chapter 1: Applied anatomy
- Chapter 2: Radiology
- Chapter 3: Congenital malformations and deformities of the cervical spine
- Chapter 4: Fractures, fracture dislocations and dislocations of the cervical spine
- Chapter 5: Soft tissue injuries of the cervical spine
- Chapter 6: Cervical spondylosis
- Chapter 7: The cervical spine in rheumatic disease
- Chapter 8: Osteomyelitis of the cervical spine
- Chapter 9: The surgical management of skeletal tumours of the cervical spine
- Chapter 10: Operations on the cervical spine
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Disorders of the Cervical Spine by Eurig Jeffreys in PDF and/or ePUB format, as well as other popular books in Medicina & Enfermedades y alergias. We have over 1.5 million books available in our catalogue for you to explore.