
eBook - ePub
Alcoholic Korsakoff's Syndrome
An Information-Processing Approach to Amnesia
- 204 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Alcoholic Korsakoff's Syndrome
An Information-Processing Approach to Amnesia
About this book
Alcoholic Korsakoff's Syndrome: An Information-Processing Approach To Amnesia presents an overview of one of the theories of amnesia, namely, the extent to which it represents an information-processing deficit. The book discusses the clinical symptoms, neuropathology, and etiology of the alcoholic Korsakoff's syndrome; the influence of the original memory model on the research in amnesia; and the functional differences among long-term memory, short-term memory, and sensory memory. The text also describes encoding deficits; the depth of encoding and visuoperceptive deficits; as well as alternative theories of amnesia. Sensory capacities and the memory and cognitive disorders of chronic alcoholics are also considered. The book further reviews the differences among various amnesic and dementing populations. Neurologist, neuropsychologists, and students taking related courses will find the book invaluable.
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedizinSubtopic
Krankheiten & Allergien1
Clinical Symptoms, Neuropathology, and Etiology
Publisher Summary
This chapter discusses the clinical symptoms, neuropathology, and etiology of alcoholic Korsakoff’s syndrome. In 1881, Carl Wernicke described a neurological syndrome in three patients that included ataxia, optic abnormalities, and confusional state. Six years following the publication of Wernicke’s paper, S. S. Korsakoff published the first of a series of reports in which he detailed the amnesic and confabulatory symptoms that often accompanied disorders involving polyneuropathy. Although long-term alcoholism often preceded these mental changes, Korsakoff noted that the symptoms also followed a number of other conditions such as persistent vomiting, typhoid fever, and intestinal obstruction. On the basis of his observations, he concluded that the presence of a substance toxic to the peripheral and central nervous systems must have been the common denominator in his reported cases. Although neither Wernicke nor Korsakoff could be specific with regard to etiology and both seemed unaware that their two syndromes often occurred sequentially in the same patients, their clinical descriptions of the symptomatology were accurate and represented important initial steps in the identification and understanding of the Wernicke–Korsakoff syndrome. The major symptoms of the Wernicke stage include a global confusional state, opthalmoplegia, nystagmus, ataxia, and polyneuropathy of the legs and arms. The Korsakoff patients’ anterograde amnesia is the most striking feature of their disorder. They are unable to learn new verbal and nonverbal information from the time of the onset of their illness.
In 1881, Carl Wernicke described a neurological syndrome in three patients (two male alcoholics, one woman with sulfuric acid poisoning) that included ataxia, optic abnormalities, and a confusional state. Postmortem examination of these three patients showed small punctate hemorrhages that were symmetrically located in the gray matter around the third and fourth ventricles of their brains. Wernicke characterized these findings, which now bears his name, as an acute inflammatory disease of the ocular–motor nuclei, and noted that the symptoms were progressive and led to death in approximately 2 weeks. Six years following the publication of Wernicke’s paper, S. S. Korsakoff published the first of a series of reports in which he detailed the amnesic and confabulatory symptoms that often accompanied disorders involving polyneuropathy. Although long-term alcoholism often preceded these mental changes, Korsakoff noted that the symptoms also followed a number of other conditions, such as persistent vomiting, typhoid fever, and intestinal obstruction. On the basis of his observations, he concluded that the presence of a substance toxic to the peripheral and central nervous systems must have been the common denominator in his reported cases. Although neither Wernicke nor Korsakoff could be specific with regard to etiology, and both seemed unaware that their two syndromes often occurred sequentially in the same patients, their clinical descriptions of the symptomatology were accurate and represented important initial steps in the identification and understanding of the Wernicke-Korsakoff syndrome.
The major symptoms of the Wernicke stage include a global confusional state, opthalmoplegia, nystagmus, ataxia, and a polyneuropathy (e.g., pain, loss of sensation, weakness) of the legs and arms. Of these neurological symptoms, the global confusional state is perhaps most germane to our interests. The patient is disoriented regarding time and place, is unable to recognize familiar people, is apathetic, inattentive, and, most significantly, is unable to maintain a coherent conversation. It is important to note that this confusional state makes assessment of memory during the Wernicke phase of an illness both difficult and of questionable validity. Memory capacities can only be assessed if it is certain that the material to be learned is attended to and comprehended, and such certainties cannot be guaranteed during the Wernicke phase of an illness. Thus, all the neuropsychological assessments described in the following chapters were conducted when the patients had passed into the chronic Korsakoff stage of their illness.
If patients with Wernicke encephalopathies are not treated with large doses of thiamine, they are in danger of having fatal midbrain hemorrhages. If, however, patients receive proper vitamin therapy, their neurological symptoms will evidence marked improvement. In most cases, the ocular problems will almost disappear, the ataxia and peripheral neuropathies will improve, and the confusional state will clear. That is, after 2 or 3 weeks of thiamine treatment, patients will realize that they are in a hospital, recognize their spouse and children, and be able to maintain an intelligible conversation with their physicians. At this point, the patients have passed the acute Wernicke phase and have entered the chronic Korsakoff stage. Very few patients in the Wernicke phase show a complete recovery to their premorbid intellectual state.
The Korsakoff patients’ anterograde amnesia is the most striking feature of their disorder. They are unable to learn new verbal and nonverbal information from the time of the onset of their illness. Learning the name of their physician, nurses, the name of the hospital, and even the location of their bed, may require weeks or months of constant repetition and rehearsal. Events that occurred hours or even minutes before will be lost to the amnesic individual. Not only do they fail to learn the names of important people and places, but often they will not remember previous encounters with these individuals. If the patients spend 3 hours completing a number of psychometric tasks, they will fail to recall the entire test session 2 hours after it has ended. Three common words read to the patient cannot be recalled 10 sec later. As one of our patients described his existence, “I always feel as though I am just waking up. I don’t remember what happened a minute ago. I don’t know the meaning of what’s going on.” Experimentally, this severe anterograde problem is exemplified by the severe difficulty the Korsakoff patient has in learning even short lists of five or six paired-associates. When alcoholic Korsakoff patients are shown a list of word pairs (e.g., man-hammer) in which they must learn to associate the second word with the first, the acquisition of these associations may require 70 or 80 trials instead of the three or four presentations needed by intact subjects.
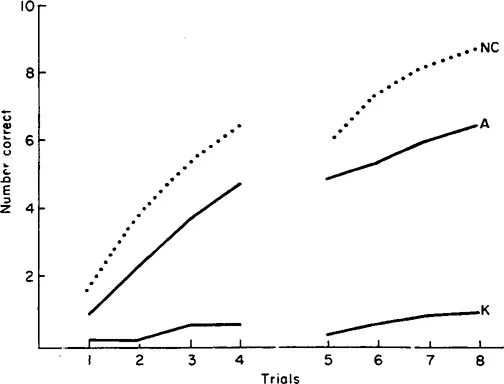
Figure 1.1 presents the results of a verbal, paired-associate learning task in which alcoholic Korsakoff patients, long-term alcoholics, and intact normal control subjects (with all groups carefully matched for age and educational background) attempted to learn a list of 10 word-pairs (Ryan, Butters. Montgomery, Adinolfi, & Didario, 1980). Although the long-term alcoholic results are inferior to those of the normal control group, both groups evidence considerable learning over the eight test trials. In fact, most of the normal controls acquire the entire 10 word-pairs by the eighth trial. The alcoholic Korsakoff patients, however, demonstrate virtually no learning during the eight trials. Their performance on Trials 7 and 8 shows little improvement over Trials 1 and 2. Such failures to learn new materials are the rule for alcoholic Korsakoff patients and remain the most obvious symptom of Korsakoff’s syndrome.
Retrograde amnesia is also a distinct and consistent feature of Korsakoff’s syndrome. The patient has trouble retrieving from long-term memory events that occurred prior to the onset of the illness. When asked who was President of the United States before Mr. Nixon, the patient might answer “Truman” or “Eisenhower.” In 1975, we asked one of our then recently diagnosed Korsakoff patients if the United States was still at war. The patient replied, “I think they have that war in Korea all wrapped up.” In general, this difficulty in retrieving old memories is usually more pronounced for events just prior to the onset of the illness, whereas remote events from the patient’s childhood and early adulthood are well remembered. Most Korsakoff patients who served in World War II can describe their tours of duty with great detail and apparent accuracy but are unable to recall any of the major historical events of the 1960s (e.g., the assassination of the Kennedy brothers, Vietnam War protests).
This temporal “gradient” is not only evident during a mental status examination but has been demonstrated in numerous experimental studies. Seltzer and Benson (1974) used a multiple choice questionnaire and found that their alcoholic Korsakoff patients could remember famous events from the 1930s and 1940s better than events from the 1960s and 1970s. Marslen-Wilson and Teuber (1975) presented alcoholic Korsakoff patients with photographs of famous people and found that the patients had much more difficulty identifying famous faces from the 1960s than faces from the 1930s and 1940s.
Warrington and her associates have challenged the existence of this gradient and have presented evidence that amnesic patients have as much difficulty retrieving remote (e.g., childhood) events as recent events. Sanders and Warrington (1971) administered a “famous events” questionnaire and a test of famous faces to five amnesics (mixed etiology). Their patients were impaired relative to the control group on all tests and for all periods of time. Unlike the impairment observed in the studies just reviewed, these patients’ impairment was of equal severity at all time periods...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- Preface
- Acknowledgments
- Chapter 1: Clinical Symptoms, Neuropathology, and Etiology
- Chapter 2: The Original Memory Model
- Chapter 3: Long-Term Memory
- Chapter 4: Short-Term Memory
- Chapter 5: Encoding Deficits
- Chapter 6: Depth of Encoding and Visuoperceptive Deficits
- Chapter 7: Alternative Theories Of Amnesia
- Chapter 8: Are All Amnesics Alike?
- Chapter 9: Sensory Capacities
- Chapter 10: Memory and Cognitive Disorders of Chronic Alcoholics
- References
- Subject Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Alcoholic Korsakoff's Syndrome by Nelson Butters,Laird S. Cermak in PDF and/or ePUB format, as well as other popular books in Medizin & Krankheiten & Allergien. We have over 1.5 million books available in our catalogue for you to explore.