eBook - ePub
Personalized Immunosuppression in Transplantation
Role of Biomarker Monitoring and Therapeutic Drug Monitoring
- 316 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Personalized Immunosuppression in Transplantation
Role of Biomarker Monitoring and Therapeutic Drug Monitoring
About this book
Personalized Immunosuppression in Transplantation: Role of Biomarker Monitoring and Therapeutic Drug Monitoring provides coverage of the various approaches to monitoring immunosuppressants in transplant patients, including the most recently developed biomarker monitoring methods, pharmacogenomics approaches, and traditional therapeutic drug monitoring.
The book is written for pathologists, toxicologists, and transplant surgeons who are involved in the management of transplant patients, offering them in-depth coverage of the management of immunosuppressant therapy in transplant patients with the goal of maximum benefit from drug therapy and minimal risk of drug toxicity.
This book also provides practical guidelines for managing immunosuppressant therapy, including the therapeutic ranges of various immunosuppressants, the pitfalls of methodologies used for determination of these immunosuppressants in whole blood or plasma, appropriate pharmacogenomics testing for organ transplant recipients, and when biomarker monitoring could be helpful.
- Focuses on the personalized management of immunosuppression therapy in individual transplant patients
- Presents information that applies to many areas, including gmass spectrometry, assay design, assay validation, clinical chemistry, and clinical pathology
- Provides practical guidelines for the initial selection and subsequent modifications of immunosuppression therapy in individual transplant patients
- Reviews the latest research in biomarker monitoring in personalizing immunosuppressant therapy, including potential new markers not currently used, but with great potential for future use
- Explains how monitoring graft-derived, circulating, cell free DNA has shown promise in the early detection of transplant injury in liquid biopsy
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Topic
MedicinaSubtopic
InmunologíaChapter 1
Overview of the pharmacology and toxicology of immunosuppressant agents that require therapeutic drug monitoring
Michael C. Milone, Hospital of the University of Pennsylvania, Philadelphia, PA, USA
This chapter provides an overview of the mechanisms of action, pharmacological parameters, reference range, and toxicological aspects of various immunosuppressants that require therapeutic drug monitoring. These immunosuppressants include cyclosporine, tacrolimus, sirolimus, everolimus, and mycophenolic acid. Chemical structures of these immunosuppressants are also provided.
Keywords
Cyclosporine; tacrolimus; sirolimus; everolimus
1.1 Introduction
More than 100,000 solid organ and 50,000 allogeneic bone marrow transplants are currently performed worldwide each year. Outcomes vary widely depending on the transplant type and underlying disease; however, solid organ allograft survival has improved significantly during the past quarter century coinciding with the introduction of new immunosuppressive drugs (ISDs). ISDs are critical to transplantation success due to the potent cellular and humoral immune mechanisms that restrict allogeneic transplantation. Whereas early ISDs consisted primarily of glucocorticoids and antimetabolite drugs to block lymphocyte proliferation, several ISDs with differing mechanisms of action have been introduced, including the recent introduction of the first biologic agent, belatacept (Nulojix, a CTLA4–Ig fusion protein), which interferes with a critical step in the initiation of T cell-mediated immunity. Although these agents have significantly improved outcomes, their benefits often come at a cost of increased risk of infection as well as toxicity. The use of ISDs to control allograft rejection and graft-versus-host disease is very difficult because errors can lead to serious and sometimes fatal consequences for the transplant recipient.
One of the greatest challenges to effectively using ISDs is their widely variable pharmacokinetic behavior across individuals. This pharmacokinetic variability makes it difficult to predict a priori an individual’s response to a drug following administration of a particular dose. Applying knowledge of a drug’s concentration and pharmacokinetic behavior within an individual to the clinical use of a drug, often termed therapeutic drug monitoring (TDM), has therefore become a standard approach to ISD therapy aimed at mitigating the risks associated with the use of these drugs. An important prerequisite to successful TDM is the ability to measure a drug of interest. Using modern technologies that are available within most analytical chemistry laboratories, the measurement of drugs, including ISDs and their metabolites, is readily achieved as described in the following chapters of this book.
Unfortunately, having the plasma or whole blood concentration of a drug is not enough for proper patient management. Effective use of drug concentration data also requires a thorough understanding of the pharmacodynamics relationship between drug exposure and important clinical outcomes of toxicity or efficacy. Like pharmacokinetics, the pharmacodynamics of ISDs also vary greatly across individuals [1], but a measured drug concentration does not provide insight into this variability. Biomarkers of organ function, tissue injury, and immune function provide some insight into the pharmacodynamics of ISDs. In the broadest sense, TDM may be considered to encompass an array of testing modalities beyond traditional concentration monitoring, such as the use of serum creatinine to monitor the nephrotoxic effects of drugs such as the calcineurin inhibitors, tacrolimus, or cyclosporine. Several of the subsequent chapters are devoted to exploring these biomarker-based testing approaches. In this chapter, the ISDs currently approved for use in solid organ and bone marrow transplantation are discussed with a focus on their pharmacology and clinical use.
1.2 Calcineurin Inhibitors
Currently, two calcineurin inhibitors (CNIs), cyclosporine and tacrolimus, are commonly used clinically as immunosuppressants. This section provides an overview of these two drugs.
1.2.1 Cyclosporine A
Introduced in the 1980s, cyclosporine A (CsA) revolutionized the care of transplant patients through its potent inhibition of acute cellular transplant rejection. Although its use has gradually been replaced by tacrolimus, it is currently used in approximately 10% of transplants. It is typically used in combination with other immunosuppressive drugs such as mycophenolic acid, azathioprine, and glucocorticoids. Originally isolated in 1969 from the soil fungus Tolypocladium inflatum by Hans Peter Frey, a biologist working at Sandoz Pharmaceuticals, CsA is a lipophilic, cyclic endecapeptide composed of N-methylated amino acids, making it resistant to intestinal digestion as shown in Figure 1.1A. It is highly lipophilic and only slightly water-soluble. It derives its primary immunosuppressive activity by selectively binding to cyclophilin A, a peptidylprolyl isomerase present within the cytoplasm of cells. Once bound, the CsA/cyclophilin complex inhibits the enzymatic activity of the calcineurin (CN), a heterodimeric, calcium-dependent serine/threonine phosphatase composed of CNA and CNB subunits that is activated by the rapid rise in intracellular calcium following T cell receptor engagement. CN removes a critical regulatory phosphorylation on nuclear factor of activated T cells (NFATc) triggering its translocation to the nucleus of T cells, where it synergizes with other factors to mediate the transcription of a large number of genes, including interleukin-2 (IL-2), an important cytokine for T cell proliferation, and CD40 ligand (CD40L), an important costimulatory ligand for B cells, as schematically diagrammed in Figure 1.1B. Although the calcineurin–NFATc pathway is critical to T cell activation, this pathway plays a role in diverse cell types, including neurons [2,3], skeletal and cardiac myocytes [4,5], and endothelium [6]. These non-immune roles of calcineurin–NFATc signaling may contribute to the toxicity observed with the clinical use of cyclosporine, which includes nephrotoxicity, neurologic toxicity (e.g., tremors and headaches), and diabetes.
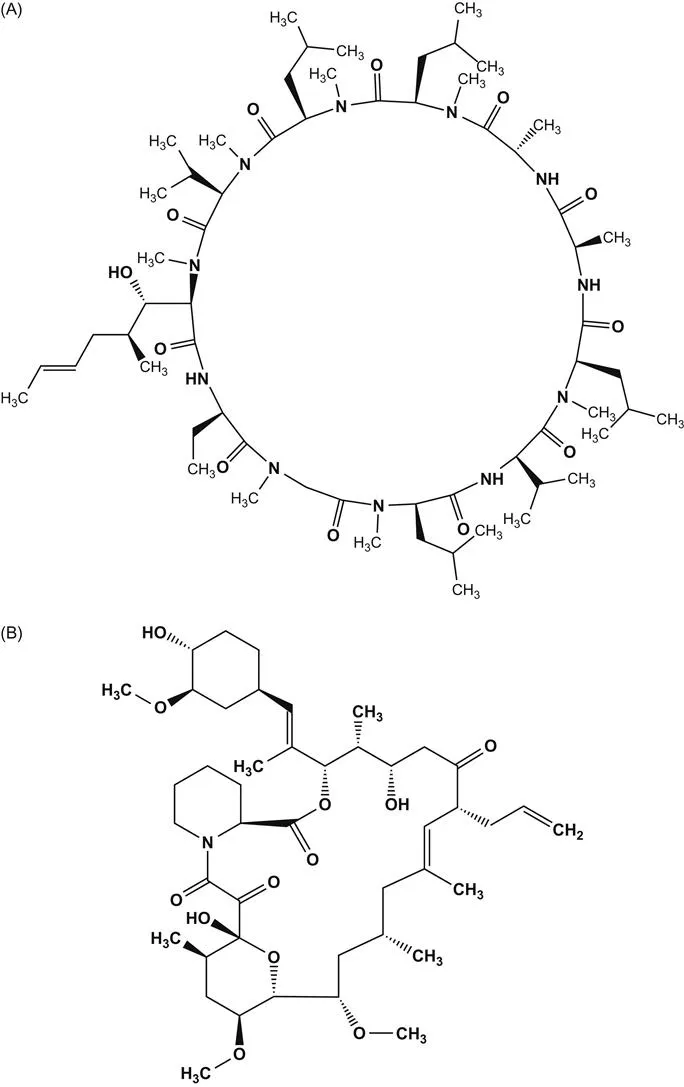
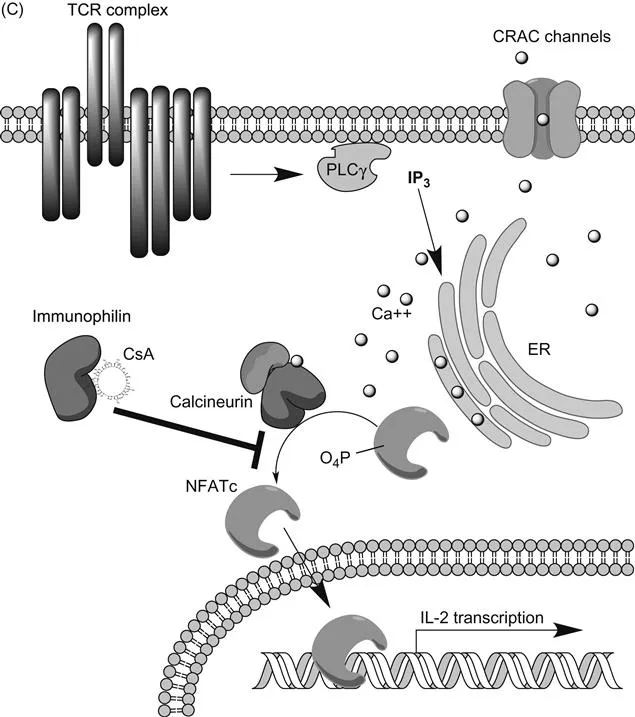
(A) Structure of cyclosporine A; (B) structure of tacrolimus;(C) schematic of calcineurin–NFATc signaling pathway in T cells that is inhibited by CsA and TRL. CRAC channel, calcium release activated channel (Orai1); PLCγ, phospholipase Cγ; IP3, inositol triphosphate.
Due to the highly lipophilic nature of CsA, the original therapeutic formulation of CsA (Sandimmune) was an oral solution of the drug dissolved in oil. This solution was then mixed with a liquid such as juice prior to consumption. Early pharmacokinetic studies revealed that CsA absorption with this formulation was slow and erratic with poor bioavailability, leading to significant intra- and interindividual variability in CsA exposure. Studies of CsA given to healthy volunteers by intravenous (IV) and oral routes demonstrated a median oral bioavailability of 21.2% [7]. CsA is highly protein bound and exhibits a large volume of distribution at steady state that ranges from 3 to 5 L/kg due to the high affinity for cyclophilins within tissues including red blood cells (RBCs) [8]. As a result of the extensive binding to RBCs, whole blood concentrations of CsA are commonly used for most pharmacokinetic (PK) studies. In addition to highly variable bioavailability, CsA also displays significant variability in clearance that spans greater than an order of magnitude (0.63–23.9 ml/min/kg) in healthy individuals [7].
Due to the poor oral bioavailability observed with these early preparations of CsA, formulations based on an oil-based microemulsion (Neoral or Gengraf) were developed in an effort to improve absorption [9]. The oral bioavailability of the microemulsion formulations was significantly improved. Bioavailability is still lower in liver transplant recipients compared to kidney transplant recipients [8]. Biliary flow and the presence of bile is a major factor affecting intestinal absorption of CsA, as illustrated by the greater than fourfold increase in bioavailability observed in liver transplant patients following T-tube clamping [10]. The improved bioavailability of CsA microemulsion is paralleled by improvements in absorption kinetics leading to a more consistent time to peak concentration and superior dose linearity with exposure. Despite these improvements in formulation, significant pharmacokinetic variability remains, with the dose-adjusted area under the concentration curve (AUC) of microemulsion-formulated cyclosporine demonstrating a greater than 20% coefficient of variation (CV) across individuals [11].
In addition to the wide variability in absorption, the variability in CsA metabolism and elimination is also clinically important. CsA is extensively metabolized to more than 25 different metabolites primarily via the cytochrome P450 3A (CYP3A) system [8,12–14]. Excretion is mostly biliary, with greater than 90% of the parent drug eliminated by this route. Renal excretion in urine accounts for only approximately 6% of drug elimination, with the vast majority excreted as CsA metabolites. As a result, renal failure has minimal effect on the clearance of CsA compared with the dramatic alterations in CsA absorption and clearance in patients with liver failure. CsA is also highly bound to cyclophilins within tissues, including RBCs. Due to the high protein binding, little CsA is also removed by hemodialysis [15]. CsA is subject to numerous drug and food interactions. Grapefruit and red wine, as well as herbal medicines such as St. John’s wort, exhibit significant interactions with CsA through their common metabolism by the CYP3A enzymatic system and membrane transport by P-glycoprotein (also known as MDR1). Commonly co-administered immunosuppressive drugs such as corticosteroids and sirolimus also show clinically relevant effects on CsA pharmacokinetics.
The relationship between CsA exposure and clinically relevant endpoints such as nephrotoxicity and organ rejection was investigated early during the use of CsA due to the highly variable pharmacokinetic behavior of the drug. In one of the earliest studies of CsA pharmacokinetics, Lindholm et al. reported on a population of 160 consecutive kidney transplant patients treated with once-daily IV or oral CsA [16]. Although transplant rejection (40%) and graft loss (23%) were significantly higher in this study compared with the incidence observed with current induction and maintenance immunosuppressive regimens, patients with higher CsA concentrations had significantly lower rates of graft rejection and higher rates of graft survival at 1 year. Subsequent studies have supported the pharmacodynamic relationship between CsA exposure and clinically relevant endpoints [17–22]. These studies have also confirmed the wide variability in pharmacokinetic behavior of this drug, particularly during the early part of the dose interval. Thus, concentration monitoring of CsA is generally considered a standard of care across transplant centers.
Although AUC0–12 h provides the best measure of drug exposure, the impracticality of making these AUC measurements, particularly in the outpatient setting, has led to the use of other surrogate measures of exposure. Because most of the variability in CsA pharmacokinetics occurs during the initial 4 h following dosing, AUC over this early post-dose period (e.g., AUC0–4 h) has been explored as a surrogate for the full-dose interval AUC0–12 h; however, even these abbreviated sampling approaches pose real challenges to collection in the clinic [22]. Pre-dose concentration (C0) represents the simplest measure of CsA exposure. Unfortunately, the correlation between C0 and AUC0–12 for CsA is relatively poor. Reported r2 (r = correlation coefficient) values for the relationship between C0 and AUC0–12 h or AUC0–4 h generally fall within the 0.4–0.6 range. C0 also appears to be a poor predictor of CsA efficacy or toxicity [17–22]. In a prospective study by Grant et al. that compared the pharmacokinetics of Neoral and Sandimmune formulations of CsA, AUC0–6 h demonstrated a significant correlation with graft rejection, with patients in the lowest quartile of AUC exposure showing a more than twofold increased incidence of rejection compared to those in the highest exposure quartile. No significant relationship betwe...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Preface
- List of Contributors
- Chapter 1. Overview of the pharmacology and toxicology of immunosuppressant agents that require therapeutic drug monitoring
- Chapter 2. Limitations of immunoassays used for therapeutic drug monitoring of immunosuppressants
- Chapter 3. Application of liquid chromatography combined with mass spectrometry or tandem mass spectrometry for therapeutic drug monitoring of immunosuppressants
- Chapter 4. Monitoring free mycophenolic acid concentration: Is there any clinical advantage?
- Chapter 5. Pharmacogenomics aspect of immunosuppressant therapy
- Chapter 6. Biomarker monitoring in immunosuppressant therapy: An overview
- Chapter 7. Graft-derived cell-free DNA as a marker of graft integrity after transplantation
- Chapter 8. Biomarkers of tolerance in kidney transplantation
- Chapter 9. Intracellular concentrations of immunosuppressants
- Chapter 10. Markers of lymphocyte activation and proliferation
- Chapter 11. Monitoring calcineurin inhibitors response based on NFAT-regulated gene expression
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Personalized Immunosuppression in Transplantation by Michael Oellerich,Amitava Dasgupta in PDF and/or ePUB format, as well as other popular books in Medicina & Inmunología. We have over 1.5 million books available in our catalogue for you to explore.