- 464 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
About this book
Gastroesophageal Reflux Disease (GERD) is one of the most common maladies of mankind. Approximately 40% of the adult population of the USA suffers from significant heartburn and the numerous antacids advertised incessantly on national television represents a $8 billion per year drug market. The ability to control acid secretion with the increasingly effective acid-suppressive agents such as the H2 blockers (pepcid, zantac) and proton pump inhibitors (nexium, prevacid) has given physicians an excellent method of treating the symptoms of acid reflux.Unfortunately, this has not eradicated reflux disease. It has just changed its nature. While heartburn, ulceration and strictures have become rare, reflux-induced adenocarcinoma of the esophagus is becoming increasingly common. Adenocarcinoma of the esophagus and gastric cardia is now the most rapidly increasing cancer type in the Western world.The increasing incidence of esophageal adenocarcinoma has created an enormous interest and stimulus for research in this area. GERD brings together a vast amount of disparate literature and presents the entire pathogenesis of reflux disease in one place. In addition to providing a new concept of how gastroesophageal reflux causes cellular changes in the esophagus, GERD also offers a complete solution to a problem that has confused physicians for over a century. Both clinical and pathological information about reflux disease and its treatment are presented. GERD is meant to be used as a comprehensive reference for gastroenterologists, esophageal surgeons, and pathologists alike.
- Outlines how gastroesophageal reflux causes cellular changes in the esophagus
- Brings together the pathogenesis of the disease in one source and applies it toward clinical treatment
- Tom DeMeester is THE leading international expert on reflux disease; Parakrama Chandrasoma is one of the leading pathologists in the area
- Book contains approximately 350 illustrations
- Ancillary web site features color illustrations: www.chandrasoma.com
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
Cell BiologyIndex
Biological SciencesCHAPTER 1
Overview of Gastroesophageal Reflux Disease
Publisher Summary
Gastroesophageal reflux is considered to be a physiological event designed to vent a stomach that becomes distended with swallowed air. The most commonly used definition of gastroesophageal reflux to assess prevalence is the presence of classical symptoms such as heartburn and regurgitation at some frequency. Another way to assess the prevalence of reflux is to determine the trends in the use of acid suppressive drugs but it is assumed that acid suppression is used mainly for reflux disease, which is only partially true. Reflux causes squamous epithelial damage as well as columnar transformation. Most patients will have pathologic changes occurring in both the squamous epithelium and the metaplastic columnar epithelium and these changes may not always be visible at endoscopy. Endoscopy performed in patients with symptomatic gastroesophageal reflux disease shows the presence of long-segment Barrett esophagus in 3% to 5% and short-segment Barrett esophagus in 10% to 15%. Patients falling into the present definition of Barrett esophagus enter long-term surveillance with regular endoscopy and biopsy to detect dysplasia or early cancer for the purpose of either preventing cancer or treating an early cancer at a stage that decreases the likelihood of death.
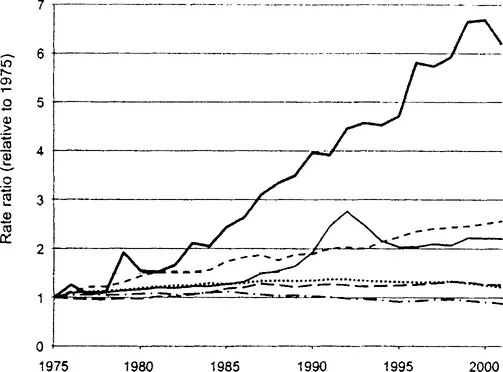
Gastroesophageal reflux disease is the classical good news-bad news story. The availability of amazingly effective acid suppressive drugs has improved the quality of life for patients by controlling pain, curing erosive esophagitis, and dramatically reducing the incidence of serious ulcers and strictures. The bad news, however, is that the incidence of adenocarcinoma induced by reflux is rapidly increasing in the United States, Western Europe, Australia, and New Zealand (1). Since the mid-1970s, the incidence of esophageal adenocarcinoma has shown the greatest increase when compared with all other cancer types (Fig. 1.1).
The detection, diagnosis, and management of patients with Barrett esophagus (BE), the precursor lesion for reflux-induced adenocarcinoma, are in a state of confusion and total disarray. It is an entity without consensus regarding definition, diagnosis, and management. This was shown very well at a recent American Gastroenterology Association workshop (2). This workshop consisted of 18 experts in the field (15 gastroenterologists, 2 surgeons, and 1 pathologist) from four countries. This group developed 42 statements on the subject of Barrett esophagus. They individually and collectively evaluated the available evidence for each statement, and after discussion they ascribed a numerical grade for the nature of the evidence (graded I to V, I being best) and level of subgroup support for the statement based on the presented evidence (A to E, A being best).
After further discussion, each expert voted his or her level of support for each statement. The grading was as follows: A = accept recommendation completely; B = accept with some reservation; C = accept with major reservation; D = reject with reservations; E = reject completely. Table 1.1 sets out the results for the 10 statements we selected as most important.
TABLE 1.1
Results of Workshop Voting for Selected Statements out of the Total of 42a
| Group Grading | |||||||
| Statement | Nature of evidence | Subgroup support | A | B | C | D | E |
| 1. Esophageal intestinal metaplasia documented by histology is a prerequisite criterion for the diagnosis of BE. | IV | C | 5 | 8 | 3 | 1 | 1 |
| 7. The proximal margin of the gastric rugal folds is a reliable endoscopic marker for the gastroesophageal junction. | IV | C | 0 | 14 | 4 | 0 | 0 |
| 9. The normal appearing and normally located squamocolumnar junction should not be biopsied. | IV | c | 14 | 4 | 0 | 0 | 0 |
| 12. Routine endoscopic screening for the detection of BE should be recommended for all adults >50 yrs of age. | V | D | 0 | 0 | 0 | 8 | 10 |
| 16. Endoscopic screening for BE and dysplasia should be performed in all adults >50 yrs of age with heartburn. | IV | D | 0 | 0 | 3 | 14 | 1 |
| 22. Endoscopic surveillance in patients with BE has been shown to prolong survival. | III | B | 0 | 5 | 4 | 8 | 1 |
| 23. Endoscopic surveillance detects curable neoplasia in patients with BE. | III | B | 7 | 8 | 3 | 0 | 0 |
| 35. Normalization of esophageal acid exposure by acid suppression reduces the risk for development of adenocarcinoma. | V | D | 0 | 0 | 2 | 9 | 7 |
| 39. In patients with BE, antireflux surgery has not proven to have a major effect against the development of adenocarcinoma. | III | A | 15 | 3 | 0 | 0 | 0 |
| 41. Mucosal ablation with acid suppression/antireflux surgery prevents adenocarcinoma in patients with BE without dysplasia. | IV | E | 1 | 0 | 0 | 0 | 17 |
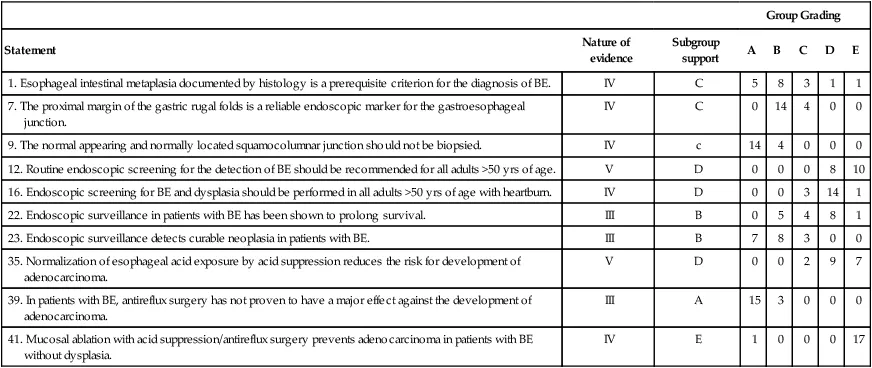
aThe statements are selected as being the most important. The group grading represents the number of experts voting for each level of support for the statement (the number is expressed as a percentage in the publication and has been converted into an absolute number).
The lack of consensus among the world’s most recognized experts for the most basic and crucial of statements regarding Barrett esophagus is astounding. There was a lack of consensus even about the most accepted of these statements such as the need for biopsy-proven intestinal metaplasia for a diagnosis of Barrett esophagus, which received a C; only 5 of 18 experts agreed completely with this statement, and 2 rejected it.
Even more amazing is the assessment of the experts regarding the nature of the evidence that exists in the literature. The experts looked at the best evidence relating to these statements and concluded that a grade IV or V was appropriate in 30 of 41 questions (grade V = insufficient evidence to form an opinion; grade IV = opinions of respected authorities based on clinical experience, descriptive studies, or reports of expert committees; grade III = evidence obtained from case series, case reports, or flawed clinical trials). The conclusion reflects an appalling state of affairs, given that these 42 statements represent the most critical that this group could come up with. Further, the wide disparity of opinion rather than consensus among the 18 experts on these important issues makes it fair to say that the understanding of this disease is in a state of total disarray and profound confusion.
The impression that we get when we read the summary of the workshop is one of great futility. Criteria for diagnosis are not agreed on, screening for the disease is generally felt to be worthless and cost-ineffective, the enthusiasm for the value of surveillance for Barrett esophagus is tepid at best (although this is a standard recommendation for patients diagnosed with Barrett esophagus), and all of today’s available treatment methods (acid suppression, antireflux surgery, and ablation) are considered ineffective in preventing adenocarcinoma.
These experts seem to be telling us that we really do not clearly know what Barrett esophagus is...
Table of contents
- Cover image
- Title page
- Table of Contents
- Preface
- Chapter 1: Overview of Gastroesophageal Reflux Disease
- Chapter 2: The Past, Present, and Future of Columnar-Lined (Barrett) Esophagus
- Chapter 3: Fetal Development of the Esophagus and Stomach
- Chapter 4: Normal Anatomy; Present Definition of the Gastroesophageal Junction
- Chapter 5: Histologic Definitions and Diagnosis of Epithelial Types
- Chapter 6: Cardiac Mucosa
- Chapter 7: New Histologic Definitions of Esophagus, Stomach, and Gastroesophageal Junction
- Chapter 8: Pathology of Reflux Disease at a Cellular Level: Part 1—Damage to Squamous Epithelium and Transformation into Cardiac Mucosa
- Chapter 9: The Pathology of Reflux Disease at a Cellular Level: Part 2—Evolution of Cardiac Mucosa to Oxyntocardiac Mucosa and Intestinal Metaplasia
- Chapter 10: Pathology of Reflux Disease at a Cellular Level: Part 3—Intestinal (Barrett) Metaplasia to Carcinoma
- Chapter 11: Pathology of Reflux Disease at an Anatomic Level
- Chapter 12: Reflux Disease Limited to the Dilated End-Stage Esophagus: The Pathologic Basis of NERD
- Chapter 13: Definition of Gastroesophageal Reflux Disease and Barrett Esophagus
- Chapter 14: Diagnosis of Gastroesophageal Reflux Disease, Barrett Esophagus, and Dysplasia
- Chapter 15: Research Strategies for Preventing Reflux-Induced Adenocarcinoma
- Chapter 16: Rationale for Treatment of Reflux Disease and Barrett Esophagus
- Chapter 17: Treatment Strategies for Preventing Reflux-Induced Adenocarcinoma
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access GERD by Parakrama T. Chandrasoma,Tom R. DeMeester in PDF and/or ePUB format, as well as other popular books in Biological Sciences & Cell Biology. We have over 1.5 million books available in our catalogue for you to explore.