eBook - ePub
Bioactive Food as Dietary Interventions for Diabetes
Bioactive Foods in Chronic Disease States
- 658 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Bioactive Food as Dietary Interventions for Diabetes
Bioactive Foods in Chronic Disease States
About this book
The role of diet in the prevention, control and treatment of diabetes continues to provide significant opportunity for non-pharmaceutical interventions for many of the over 20 million people who live with this disease. Looking beyond traditional dietary controls may lead to more effective, cost efficient, and flexible options for many patients.
Bioactive Food as Dietary Interventions for Diabetes is the only available scientific resource focused on exploring the latest advances in bioactive food research, and the potential benefit of bioactive food choice on the diabetic condition. Written by experts from around the world, it presents important information that can help improve the health of those at risk for diabetes and diabetes related conditions using food selection as its foundation.
- Focuses on the role of bioactive foods in addressing pre-diabetes symptoms, their potential to complement other treatments for those suffering from diabetes and diabetic-related obesity and other health issues
- Documents foods that can affect metabolic syndrome and ways the associated information could be used to understand other diseases that share common etiological pathways
- Includes insights from experts from around the world, providing global perspectives and options based on various regional foods
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Subtopic
Endocrinología y metabolismoChapter 1
Role of Oxidative Stress in the Pathogenesis of Insulin Resistance and Type 2 Diabetes
Abbreviations
ALA α-lipoic acid
AMPK AMP-dependent protein kinase
ER Endoplasmic reticulum
FFA Free fatty acids
GLUT-4 Glucose transporter isoform-4
GSK-3 Glycogen synthase kinase-3
GSV GLUT-4-sequestering vesicle
H2O2 Hydrogen peroxide
HGP Hepatic glucose production
IKK I-kappa kinase
IR Insulin receptor
IRS Insulin receptor substrate
JNK c-jun N-terminal kinase
LDL Low-density lipoprotein
MAPK Mitogen-activated protein kinase
NO Nitric oxide
PDK Phosphoinositide-dependent kinase
PI3-kinase Phosphotidylinositol-3-kinase
PKC Protein kinase C
RAS Renin–angiotensin system
ROS Reactive oxygen species
1 Introduction
Type 2 diabetes, defined as a fasting plasma glucose level above 126 mg dl−1, is a devastating disease of defective regulation of whole-body glucose homeostasis that leads to the development of myriad complications, including retinopathy and a greater risk of blindness, nephropathy and increased risk of kidney failure, neuropathy and increased risk of limb amputation, and accelerated coronary, cerebral, and peripheral vascular damage and enhanced risk of heart attack and stroke. The prevalence of type 2 diabetes in the United States is increasing dramatically, with an estimated 26 million Americans suffering from this disease in 2011. A critical underlying defect that is associated with the development of type 2 diabetes and its immediate precursor, termed prediabetes, is a decreased ability of insulin to regulate glucose metabolism in peripheral insulin-sensitive tissues, including skeletal muscle, adipose tissue, and liver, and in the hypothalamus of the central nervous system (Henriksen, 2002). This diminished insulin action is referred to as insulin resistance, and the multifactorial etiology of insulin resistance has been the focus of hundreds of basic science and clinical investigations over the past decades.
As stated earlier, there are numerous potential underlying causes for the development of insulin resistance in various organs, and a comprehensive review of all of these factors is beyond the scope of this chapter. This chapter is therefore organized into the following sections: first, a brief overview of the normal regulation of systemic glucose homeostasis resulting from the interplay among several organ systems is described. Thereafter, the basics of the defects in insulin signaling that underlie most states of insulin resistance are reviewed. The focus of the remainder of the chapter is placed on the role of the specifically deleterious condition termed oxidative stress in the etiology of defective insulin action, especially in skeletal muscle. A corollary to this coverage of oxidative stress-associated insulin resistance is a brief discussion of the utility of antioxidant interventions to ameliorate this specific type of defective insulin action.
2 Systemic Glucose Homeostasis is a Multiorgan Process
The overall regulation of plasma glucose levels (70–100 mg dl−1 in the short-term fasted state) is a function of the concerted contributions of several organ systems in the body, including skeletal muscle, liver, adipose tissue, the alpha- and beta-cells of the endocrine pancreas, and specialized neurons in the hypothalamus (Figure 1.1). The secretion of insulin from the beta-cells of the endocrine pancreas is regulated primarily by the circulating level of glucose that is detected by these cells and coupled, via a multistep process, to the exocytosis of insulin-containing vesicles. This glucose-linked insulin secretion can be modified by several other inputs to the beta-cells, such as glucagon secreted from adjacent alpha-cells in the pancreas (promoting insulin secretion), sympathetic (inhibitory) and parasympathetic (stimulatory) neural input, and incretins such as glucagon-like peptide-1 (stimulatory) secreted primarily from L-cells located in the intestine.
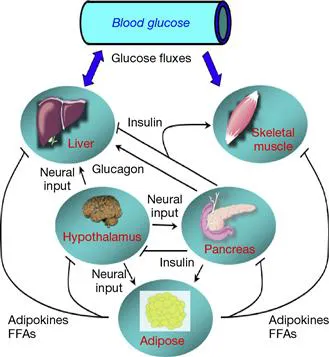
Figure 1.1 Interactions of organ systems in the regulation of systemic glucose concentrations.
Skeletal muscle, which makes up ~40% of body mass in most individuals, is a major site of insulin-dependent glucose disposal, and is a critical site of defective insulin action that can lead to the development of type 2 diabetes. In this context, skeletal muscle is the focus of discussion in this chapter. Insulin acts on the insulin receptor (IR) in the plasma membrane of skeletal muscle cells to stimulate a series of intracellular signaling events that ultimately result in the translocation of the glucose transporter isoform-4 (GLUT-4), located in intracellular GLUT-4-sequestering vesicles (GSV), to the plasma membrane, where the GLUT-4 can promote glucose transport via a facilitative diffusion mechanism (Henriksen, 2002), the major mechanism in myocytes for enhanced glucose transport activity (Guma et al., 1995). There are several proteins involved in the canonical insulin signaling pathway. Following insulin binding to the exofacial alpha-subunit of the IR and the associated activation of tyrosine kinase activity of the transmembrane beta-subunits, several intracellular proteins can be phosphorylated on tyrosine residues, such as IR substrates (IRS) 1 and 2. The conformational changes elicited by this tyrosine phosphorylation allow IRS-1 and IRS-2 to interact and activate phosphotidylinositol-3-kinase (PI3-kinase). PI3-kinase can then produce phosphoinositide moieties that allosterically activate 3-phosphoinositide-dependent kinases (PDK), a serine/threonine kinase. One isoform of the PDK (PDK1) can activate Akt by Thr308 phosphorylation. Akt can also be phosphorylated on Ser473 and activated by engagement of the mTOR complex 2 (Kleiman et al., 2009). This activated Akt can subsequently phosphorylate and inactivate the Rab-GTPase-containing AS160, also known as TBC1D4, thereby allowing movement of GSVs to the plasma membrane and initiating facilitated glucose transport via GLUT-4 (Cartee and Wojtaszewski, 2007). Phosphorylation of IRS proteins by several serine kinases also represents an aspect of normal dampening of IRS activity by insulin action; however, insulin resistance can be caused by overactivity of these serine kinases, as expanded upon later.
The contribution of the other aforementioned organ systems to overall glucose homeostasis will now be covered in brief. The liver is the major site of de novo glucose production and release into the circulation (Wasserman and Cherrington, 1991). Insulin is the primary endocrine factor for suppression of hepatic glucose production (HGP) and glucagon is the primary endocrine factor for stimulation of this process. Therefore, the ratio of the concentration of glucagon to insulin in the hepatic portal circulation is a critical determinant of HGP (Wasserman and Cherrington, 1991). Insulin will also exert a powerful effect to inhibit lipolysis in adipose tissue, thereby reducing release of free fatty acids (FFA), which normally inhibit insulin action in skeletal muscle and liver (Reaven, 1995).
Adipose tissue is also a critical site of the synthesis and release of myriad proteins, called adipokines or adipocytokines, that impact the functionality of numerous organ systems, including skeletal muscle and liver (Lee et al., 2009). The majority of adipokines elicit a negative action on insulin-dependent processes in skeletal muscle and liver. In contrast, one adipokine, called adiponectin, has the effect to enhance the action of insulin to stimulate glucose transport activity in skeletal muscle and to facilitate glycogen synthesis in both skeletal muscle and liver. In general, as adipose tissue mass expands in the development of obesity, the release of the deleterious adipokines increases and the release of adiponectin decreases, changes that can mechanistically contribute to insulin resistance in skeletal muscle and liver (Lee et al., 2009).
Finally, the hypothalamus contains specific neurons that respond to neural, endocrine, and nutrient inputs (such as insulin, glucose, and FFAs), and can, in turn, regulate the secretion of insulin and glucagon from the pancreas, glucose production by the liver, and release of FFAs from adipose tissue (Lee et al., 2009). In this fashion, the hypothalamus plays a critical role in the neural control of the organ systems that contribute to overall glucoregulation.
3 Glucose Dysregulation: The Pathogenesis of Insulin Resistance
Dysfunctions in the organ systems reviewed earlier, especially in skeletal muscle, are associated with an impaired ability to maintain fasting plasma glucose within a tolerable range and to respond appropriately to oral glucose challenges, as occurs following the ingestion of a meal or beverage containing carbohydrates. The underlying mechanisms for these dysfunctions, with a focus on skeletal muscle, will be discussed in this section of the chapter.
The progression to a state of overt type 2 diabetes, hallmarked by elevated fasting plasma glucose and impaired glucose tolerance, depends initially upon the development of insulin resistance, primarily in skeletal muscle and liver, combined with a reduction in the capacity of beta-cells to secrete sufficient insulin to compensate for this insulin resistance (DeFronzo, 2009; Reaven, 1995). In skeletal muscle, quantitatively the most important site of glucose disposal and a critical contributor to whole-body glucose homeostasis, insulin resistance is associated with defects in the ability of insulin to stimulate the translocation of GLUT-4 to the plasma membrane and facilitate glucose transport into the myocytes (Henriksen, 2002). This impairment in insulin-dependent GLUT-4 translocation arises primarily from multifactorial defects in the normal engagement of the canonical insulin signaling cascade (Henriksen, 2010).
A key contributor to this reduced flux through the insulin signaling cascade to initiate GLUT-4 translocation is elevated serine phosphorylation of both the IR and the IRS proteins (Henriksen, 2010), the initial elements of this pathway. A number of serine kinases are known to act on the IR and IRS proteins, including atypical protein kinase C (PKC) isoforms, Akt, glycogen synthase kinase-3 (GSK-3), the mitogen-activated protein kinases (MAPK or ERK1/2), c-jun N-terminal kinase (JNK), I-kappa kinase-β(IKKβ), and p70S6 kinase, among others (Henriksen, 2010). Elevated serine phosphorylation of the IR and the IRS proteins is associated with a reduction in tyrosine phosphorylation and a concomitant diminution of the functionality of these signaling elements, with diminished engagement of downstream factors in this insulin signaling cascade.
Insulin resistance in the liver, with a reduced ability of insulin to suppress HGP and stimulate glycogen synthesis, results from a similar dysfunction in the regulation of the IR, the IRS proteins, and downstream insulin signaling, such as Akt. Much less is known about the etiology of insulin resistance in the hypothalamus (DeFronzo, 2009).
The next sections of this chapter will review the specific role of oxidative stress in the etiology of insulin resistance and the utility of antioxidant interventions to ameliorate oxidant stress-associated insulin-resistant states.
4 Origins of Oxidative Stress in Various Cell Types
Oxidative stress can be defined as an imbalance in cells or in plasma between the production of various oxidants and the antioxidant mechanisms for removal of these excess ox...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Preface: Diabetes Food
- Contributors
- Chapter 1. Role of Oxidative Stress in the Pathogenesis of Insulin Resistance and Type 2 Diabetes
- Chapter 2. Diabetes and the Role of Dietary Supplements
- Chapter 3. Government Regulation of Dietary Supplements and Foods: Role in Diabetes
- Chapter 4. Diabetes as an Immune Dysfunction Syndrome
- Chapter 5. Antihyperglycemic Potential of Secoisolaricinol Diglucoside
- Chapter 6. Antidiabetic Potential of Trigonelline and 4-Hydroxyisoleucine in Fenugreek
- Chapter 7. Community Participation and Diabetes Control
- Chapter 8. Glycine max (Soybean) Treatment for Diabetes
- Chapter 9. Amino Acid Supplements and Diabetes
- Chapter 10. Reduction in Serum Glucose with Garlic Extracts
- Chapter 11. Dietary Supplements, Immune Modulation, and Diabetes Control
- Chapter 12. Dietary Supplements and Herbs in Diabetes and Its Prevention
- Chapter 13. Phytotherapeutics in Treating Diabetes
- Chapter 14. Plant-Derived Hydroxycinnamate Derivatives, Insulin Sensitivity, and Adiponectin: Implications for Diabetes Control
- Chapter 15. Antidiabetic Activity of Allium Sativum
- Chapter 16. Chromium and Diabetes
- Chapter 17. Dietary Calcium and Magnesium and the Risk of Type 2 Diabetes
- Chapter 18. Polyunsaturated Fatty Acids and Insulin Resistance
- Chapter 19. Vitamin D and Type 2 Diabetes Mellitus
- Chapter 20. Pongamia pinnata: Treatment of Diabetes
- Chapter 21. Oyster Mushroom (Pleurotus pulmonarius) and Diabetes Care
- Chapter 22. Traditional Medicinal Plants of Indigenous Peoples of Canada and Their Antioxidant Activity in Relation to Treatment of Diabetes
- Chapter 23. Indian Medicinal Plants with Hypoglycemic Potential
- Chapter 24. Plant Extracts and Alkaloids: Prevention of Diabetic Nephropathy
- Chapter 25. Lutein and Diabetic Cataracts
- Chapter 26. Compounds in Vegetables Including Okra and Fenugreek of Potential Value in the Treatment of Diabetes
- Chapter 27. Probiotics and Diabetes/Obesity: Health Implications
- Chapter 28. Tradition and Perspectives of Diabetes Treatment in Greco-Arab and Islamic Medicine
- Chapter 29. State of the Art of Diabetes Treatment in Greco-Arab and Islamic Medicine
- Chapter 30. Phytonutrients in Diabetes Management
- Chapter 31. Antidiabetic Effects of Punica granatum L (Pomegranate): A Review
- Chapter 32. Type II Diabetes Mellitus: 2011 Research Summary
- Chapter 33. Diabetes and Natural Products
- Chapter 34. L-Carnitine in Patients with Diabetes
- Chapter 35. Antioxidants and Inflammation in Obesity
- Chapter 36. Magnesium and Metabolic Syndrome: The Role of Magnesium in Health and Disease
- Chapter 37. Obesity in Ayurveda: Dietary, Lifestyle, and Herbal Considerations
- Chapter 38. The Effects of a Fermented Soy Product and Isoflavones in Metabolic Syndrome Control
- Chapter 39. Anti-Inflammatory Actions of Pycnogenol: Diabetes and Arthritis
- Chapter 40. Metabolic Syndrome: Diet, Obesity, and Chronic Inflammation
- Chapter 41. The Indian Medicinal Plant Aegle marmelos in the Treatment of Diabetes Mellitus: Promise and Prospects
- Chapter 42. Antidiabetic and Hypoglycemic Effects of Syzygium cumini (Black Plum)
- Chapter 43. Human Milk as a Bioactive Food
- Chapter 44. Ginger (Zingiber officinale Roscoe) in the Treatment of Diabetes and Metabolic Syndrome: Preclinical Observations
- Chapter 45. Antidiabetic and Cardioprotective Effects of Amla (Emblica officinalis Gaertn) and its Phytochemicals: Preclinical Observations
- Chapter 46. Prickly Pear Cactus (‘Nopal’) for the Treatment of Type 2 Diabetes Mellitus
- Chapter 47. Antioxidant Capacity of Honey: Potential Health Benefit
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Bioactive Food as Dietary Interventions for Diabetes by Ronald Ross Watson,Victor R Preedy,Victor R. Preedy in PDF and/or ePUB format, as well as other popular books in Tecnología e ingeniería & Endocrinología y metabolismo. We have over 1.5 million books available in our catalogue for you to explore.