1
Ultrasound in Assisted Reproductive Technology: Anatomy and Core Examination Skills
Nazar N. Amso
Introduction
Ultrasound imaging has extensive applications in medicine, and these continue to evolve [1]. Its influence on gynecological practice has been transformational. The practice has become more office and ambulatory based for several reasons, namely, a more efficient and cost-effective service associated with higher patient satisfaction. Although both transabdominal sonography (TAS) and transvaginal or endovaginal sonography (TVS) have been available for many decades [2], it is the transvaginal route that has by far been the most influential on practice. This is due to (1) the higher frequency of the transvaginal transducer in comparison with the transabdominal one (6–8 MHz versus 2–6 MHz) resulting in better image resolution, (2) proximity of the ultrasound emitting tip of the probe to the region of interest, i.e., the pelvis, and (3) the ability to undertake many procedures through the vaginal route under direct ultrasound guidance without the need for general anesthesia.
Hence, ultrasound, as a noninvasive tool, is now the modality of choice for the assessment of normal and abnormal pelvic anatomy. It is ideal to image the uterine morphology and dimensions, ovaries, urinary bladder, adnexa, anal sphincter, and retroperitoneal space. At present, TAS and TVS are used in a variety of settings, e.g., in early pregnancy assessment, outpatient and reproductive health clinics, gynecologic oncology, adolescent gynecology, urogynecology, infertility, and postmenopausal gynecology [4]. The introduction of three-dimensional (3D) ultrasound has further increased the diagnostic role of TVS for uterine malformations. Many of these applications are explored in detail in other chapters of this book.
The acceptability of TVS was previously reported [3,4]. Most women undergoing TVS dating scans described no or mild discomfort (52% and 47.5%, respectively), while 0.7% experienced marked discomfort. In the same study, 88% of women accepted TVS, and 95% said that they would have no concerns about another TVS in a future pregnancy [5]. These findings were confirmed by a more recent study [6].
Ultrasound remains very subjective and operator dependent. The increasing applications and greater availability of cheaper general-purpose portable ultrasound machines necessitate adequate training in the technique and interpretation of the acquired images before commencing independent practice. In this chapter, the author focuses on the TVS technique and the appearance of the normal pelvis, as it is the most relevant to infertility practice. Other chapters expand on abnormal findings in the nonpregnant and pregnant states.
Know Your Anatomy
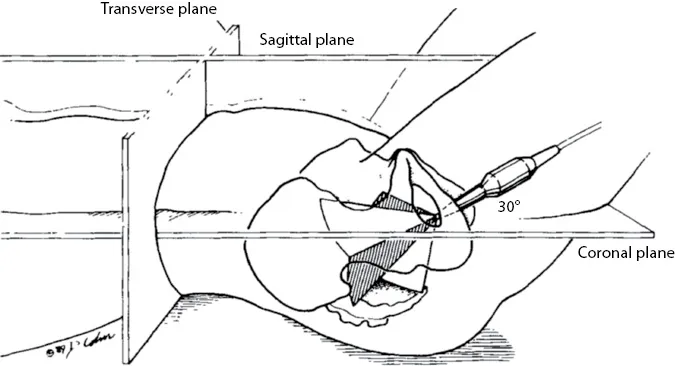
There is need for clarity in describing the anatomical planes used to obtain images during TVS. The conventional anatomical planes nomenclature used in anatomy or radiology, namely, sagittal, transverse, and coronal, do not generally correspond closely with the anatomical planes in TVS. Several factors should be considered; the transducer is inserted into the vagina, which runs in a downward and posterior direction, and the pelvis is tilted at an angle 30° to the long axis of the body; the vaginal walls and vaginal vault limit the depth and range of hand movement employed to obtain the images; and limitations imposed by the angle of view, transducer position, and image magnification lead to incomplete assessment of a pelvic plane in one image [8]. Hence, the transducer is continually manipulated in various directions to assist the operator in acquiring relevant information to form a virtual 3D image of the pelvis.
The sagittal plane, also referred to as median or longitudinal, runs along the long axis of the body dividing it into right and left halves and is at right angles to both the coronal, also called frontal, and transverse planes. These respectively divide the body into front and back parts and upper and lower parts (Figure 1.1) [7].
Figure 1.1 The three anatomical planes of the human body and their relationship to the ultrasound beam during transvaginal scanning. The transverse plane is at right angles to the long axis of the body; the coronal plane is at right angles to the median plane in the longitudinal axis passing through the coronal sutures (and generally includes planes parallel to the planes passing through the coronal sutures); and the sagittal plan is parallel to the median plane passing through the sagittal sutures (planes parallel to the...