
- 330 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Waking and the Reticular Activating System in Health and Disease
About this book
Waking and the Reticular Activating System in Health and Disease provides a comprehensive overview on the "activating properties of the RAS. In health, the RAS provides the basis against which we assess the external world, and in disease it distorts that world and shatters our self-image. This book describes the physiology of each process, how it is disturbed in each disorder, and what the most appropriate treatment should be.
Dr. Garcia-Rill, along with contributions from leading specialists, discusses the understanding of the RAS as a system not only modulating waking, but also in charge of survival mechanisms such as fight vs flight responses and reflexes. The full spectrum of these functions helps explain the complexity of symptoms evident in such disorders as disparate as schizophrenia and Parkinson's disease. The book reviews the mechanisms that control waking and arousal, and especially how those mechanisms malfunction in certain neurological and psychiatric disorders.
- First comprehensive overview on the RAS and its role in schizophrenia, major depression, autism, Parkinson's, Alzheimer's, and other neurologic and mental diseases
- Offers a new way of thinking about brain function and the role of the RAS in our waking lives
- Written by a leading translational neuroscience researcher with contributions by specialists in the field
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
Governing Principles of Brain Activity
Edgar Garcia-Rill, PhD Center for Translational Neuroscience, Department of Neurobiology and Developmental Sciences, University of Arkansas for Medical Sciences, Little Rock, AR, USA
Abstract
When we awaken, the world is instantaneously in harmony. We are ourselves once again and pick up exactly where we left off the day before. Although many books deal with sleep and sleep disorders or waking functions like attention, learning, and memory, very few books address waking itself and the process of staying awake. Our brains provide the “content” of sensory experience, but a second element is required for perception, the “context” of sensory experience. This often-ignored part of our sensory experience is provided by the reticular activating system and, without it, we cannot appreciate or perceive the world around us.
Keywords
Cell assemblies
Coherence
Cortical columns
Frequency
Thalamocortical dysrhythmia (TCD)
Thalamocortical resonance
Why Waking?
When we awaken, the world is instantaneously in harmony. We are ourselves once again, no matter what nonsense we have been dreaming. We pick up exactly where we left off the day before, the memories flooding in about the day's tasks. What does it take to wake up and, more importantly, to stay awake? This is an underappreciated faculty, yet when we lose it, we disappear. When we fall asleep, are anesthetized, or become comatose, our sense of self vanishes. There is nobody home. We have no memory when we are in slow-wave sleep (SWS), when we are anesthetized, or when we are comatose. There is a neurological condition in which this happens gradually. In Alzheimer's disease, patients seem to slowly, inexorably, lose their sense of self. On the other hand, we have some memory of our dreams. During sleep, every 90 min or so, we transition from SWS to rapid eye movement (REM) sleep. It is during this time that we dream. When we dream, we are mostly ourselves, but sometimes someone else, and we are in a distorted world, at times enjoyable and at times fearsome. Only our eyes live out our dreams because our extraocular muscles are not paralyzed, but the rest of the body is thankfully paralyzed, this is the atonia of REM sleep. Our frontal lobes have low blood flow so we are not exactly the sharpest tacks in the box. That is, we have little critical judgment, so that our dreams run the gamut of recalled and manufactured experiences. We believe the surrealistic collage of feelings and situations in dreams and accept them at face value no matter how crazy or unreal. We basically are suffering from a hallucination, but thankfully, we cannot act dreams out because of the atonia of REM sleep. There is a neurological condition in which our bodies are not paralyzed when we dream. If our bodies are not paralyzed while we dream, we begin to act out our dreams. We begin to fight perceived enemies, although they may be our unrecognized bed partners. We can cause them physical harm and we can persist until awakened by force. This occurs when we suffer from REM sleep behavior disorder, a rare disease discovered by the brilliant psychiatrist Carlos Schenck and his equally eminent neurologist codiscoverer Mark Mahowald (Schenck et al., 1987).
We spend a third of our lives asleep, about 80–85% of that in SWS, and the rest in REM sleep. However, we spend two-thirds of our lives awake. Waking is when we develop ideas, create objects, develop relationships, interact with other people, and earn a living, basically, when we do the really important things in life. Despite the importance of waking, there are very few books about waking and the process of staying awake. There are many books about sleep and about sleep dysregulation, about what happens when we have abnormal sleep, and when our vigilance interrupts or pushes aside our sleeping hours. The complaints patients tender are usually “problems sleeping,” hardly ever do they say they have “problems waking.” But the fact is that most psychiatric and neurological disorders involve just that, “problems waking.” That is, hypervigilance and increased REM sleep drive cut down on our sleep, waking us early, often when we suffer from these diseases. We will address this issue in Chapter 2. In a number of other chapters, we will see how the process of waking has begun and how it is maintained. Without a firm understanding of the mechanisms behind waking, treating and controlling the so-called sleep disorders become more difficult. A firm grasp of the regulation of waking will also allow much better comprehension of the hyperarousal problems in a number of psychiatric and neurological disorders. In the following chapters, we will see how this process is disturbed by disease. Part of the problem is that we hardly ever study the process of waking per se.
The Gorilla in the Room
There is a major difference between the real world and our studies of the human brain. In the real world, we are under continuous sensory load and always processing varied information. In the lab, our brain is studied under “controlled” conditions, that is, we are only subjected to a single stimulus at a time and we are required to elicit a response in a fixed manner. The real world is messy and complex, while the lab is neat and sterile. An animal in nature is exploring the environment, is bombarded by sensations, is exposed to multiple perceived threats, is repeatedly calculating fight-or-flight responses, and is planning the next meal. A laboratory subject is sitting still, probably listening to a background of white noise, and waiting for a stimulus to which to respond. The highest threat is the fear of falling asleep. Under these conditions, most sensory and motor physiologists ignore the gorilla in the room. They ignore the level of arousal, the stream of afferent information that establishes the background of activity upon which we normally superimpose our sensations, responses, and desires. Similarly, studies in animals do not take into account the excitability level of the subject. While real life is equivalent to listening to a concert played by many instruments emitting a myriad of notes, the laboratory setting is like sitting in a silent room and listening to a single note.
We have used such “controlled” conditions to dissect many basic principles and have acquired a host of information. Our need to determine cause and effect has led us to reduce experimental conditions to the smallest common denominator. This has been a productive approach to date, but we now need to study not only the “content” of sensory information but also the “context” under which we perceive that information. We have been very successful at determining very basic principles of brain function and have made great inroads into how the brain perceives simple stimuli and events. That is, we have been productive at discerning the responses to the “content” of sensory experience. However, we hardly address the other half of conscious perception, the “context” under which we perceive and act. While this may seem a lesser endeavor, the point will be made that, experimentally speaking, we ignore the majority of our waking world. How does the background of activity change the perception of sensory events? Are the responses the same when we are sedentary compared to when we are active? It would seem that the stimulus may be the same, but the consequent responses are markedly different when superimposed on a complex, continuously varying background. Are these consequences the same after being exposed again to the same stimulus, or do they change over time as the background of activity changes? The responses are probably considerably different, but we have little idea in what way they are different.
When we are awake, a mild auditory stimulus such as a voice produces a response that can be recorded in the auditory cortex. That same response is produced in the cortex if we are asleep. That is, the evoked response at the level of the cortex to the same sound stimulus is similar, yet we do not respond when we are asleep and we do respond when we are awake. If the sensory input produces a similar signal at the level of the cortex whether we are asleep or awake, what is the difference? The difference is the “context” under which we perceive the input during waking. While asleep, low-frequency activity in the electroencephalogram (EEG) does not lead to significant recognition or meaning to the sound received, despite the activation of the cortex by the sensory event. During waking, the background of activity, of high-frequency oscillations, leads to the recognition and integration of the stimulus into ongoing brain activity (Llinás and Paré, 1991). We can think of this like two gears, an internal gear that rotates in concert with the ongoing activity of the brain and an external gear that rotates with the input coming from the external world. When we are awake, the internal and external gears mesh and the internal and external worlds are merged seamlessly. They both rotate at gamma band frequency (~ 40 Hz) and provide unity to perception. When we are asleep, especially during SWS, the internal gear does not mesh with the external gear and is in fact rotating more slowly, at delta-band frequency (~ 4 Hz), than the external gear. External inputs do not force the gears to mesh unless the external input is stronger, strong enough to activate the reticular activating system (RAS). Only then does the external world intrude enough to make the gears mesh and rotate at the same rate. Only then does the arousing input awaken us to help drive the internal gear at gamma band frequency. We will see in Chapter 10 how the “context” of our sensory experience even drives our voluntary movements (Figure 1.1).
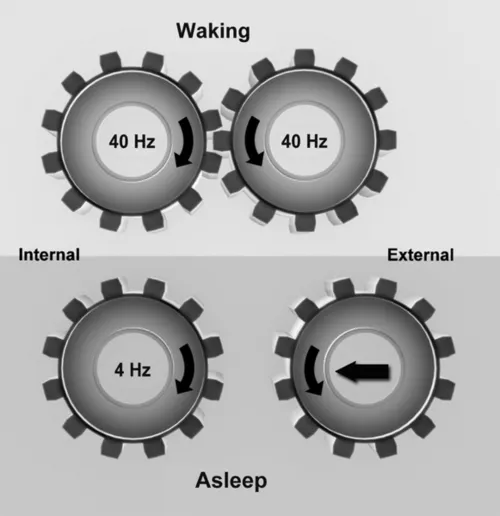
Figure 1.1 Internal and external gears during waking and sleep. Top: During waking, internal brain circuits generate high-frequency (beta/gamma) activity. These are in synchrony with the high-frequency activity generated by sensory afferents to the brain. The internal and external worlds are coherent. Bottom: During sleep, the internal gear slows to delta in the absence of high-frequency activity and the external gear is uncoupled, making awakening more difficult. During REM sleep, the internal gear generates high-frequency activity in the absence of a link to the external world. Coupled with decreased frontal lobe blood flow during REM sleep, critical judgment is absent and the brain is free to “manufacture” plots without realistic anchor. Fortunately, our muscles are paralyzed by the atonia of REM sleep that keeps us from acting out these plots. Only our eye muscles have sufficient muscle tone to live out our dreams, thus the presence of REMs.
What happens during REM sleep? The sensory input does not reset the ongoing gamma band oscillations of REM sleep so that the afferent information is not placed in “context” with the internal state of the system (Llinás and Paré, 1991). That is, the internal gear is rotating at gamma frequencies but totally disconnected from the external gear. We typically awaken during the last REM sleep episode of the night. Our RAS is already activated (the internal gear is rotating at ~ 40 Hz but disconnected from the external gear), and it is only a slight additional activation that shifts us from REM sleep to waking. If we are in SWS, it typically requires a strong stimulus to awaken us. Our brains are not as activated so that it seems that we are disoriented when we are awakened from a SWS episode. These considerations do not simply apply to normal, ongoing waking function, but they are involved in the disease process. Imagine a disease in which the two gears are rotating at slightly different speeds. The perceptual distortions would be disturbing. Imagine a disease in which a cog is missing and meshing “skips” on a regular basis. The dissonance between the internal world and the external environment is the basis for a number of neurological and psychiatric disorders. Many of the disorders we will consider are characterized by decreased or interrupted gamma band activity. But before we consider such concepts, we need to understand some basic principles of brain function.
Cell Assemblies
Donald Hebb synthesized certain ideas on how the environment and experience can influence brain structure and function (Hebb, 1949). He postulated the presence of cell assemblies in the brain that would fire as a consequence of sensory input to produce a sensation and that the activity would persist in the assembly and would represent the concept of the input. If the input occurred often, the circuit would be reinforced by the strengthening of synapses within that circuit and establish what he termed a “phase sequence.” He proposed, “Any frequently repeated, particular stimulation will lead to the slow development of a “cell assembly,” a diffuse structure comprising of cells in the cortex and diencephalon (and also, perhaps, in the basal ganglia of the cerebrum), capable of acting briefly as a closed system, delivering facilitation to other such systems and usually having a specific motor facilitation. A series of such events constitutes a ‘phase sequence’—the thought process” (Hebb, 1949).
This concept became the bedrock of experimental investigation and the starting point for discussion of perception, attention, intelligence, learning, memory, and mental illness, among other subjects. The evidence for cell assemblies, or neural nets that behave the same way, is considerable, with results showing that the electrical activity of groups of neurons corresponds to the process of perception. We will see later that this involves gamma band activity or the “40 Hz rhythm.” Hebb proposed (1) that the reverberation of activity around the cell assembly depended only on excitation and (2) that the synchronized activity throughout the circuit depended only on the synaptic connectivity. These have been recognized as limitations to Hebb's theory...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Acknowledgments
- Dedication
- Preface
- Chapter 1: Governing Principles of Brain Activity
- Chapter 2: The EEG and the Discovery of the RAS
- Chapter 3: Other Regions Modulating Waking
- Chapter 4: Wiring Diagram of the RAS
- Chapter 5: Development and the RAS
- Chapter 6: Ascending Projections of the RAS
- Chapter 7: Descending Projections of the RAS
- Chapter 8: The 10 Hz Fulcrum
- Chapter 9: Gamma Band Activity
- Chapter 10: Preconscious Awareness
- Chapter 11: Psychiatric Disorders and the RAS
- Chapter 12: Neurological Disorders and the RAS
- Chapter 13: Drug Abuse and the RAS
- Chapter 14: The Science of Waking and Public Policy
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Waking and the Reticular Activating System in Health and Disease by Edgar Garcia-Rill in PDF and/or ePUB format, as well as other popular books in Biological Sciences & Neurology. We have over 1.5 million books available in our catalogue for you to explore.