eBook - ePub
About this book
Researchers' knowledge of gliomas continues to advance rapidly at both the basic and translational levels, and Gliomas provides a thorough overview of the evolving fields of tumor biology and clinical medicine as they relate to our understanding of brain tumors.
Gliomas reviews the current paradigms that underlie these fields, beginning with the molecular epidemiology of glioma susceptibility and prognosis through population-based science and genome-wide association studies. The book's discussion of imaging modalities extends beyond advances in anatomical imaging to include metabolic and physiological studies. This work provides thorough discussion of the clinical view of tumors, ranging from the presentation of the patient to surgical management, and covers all therapeutic options for patient care, including chemotherapy, targeted molecular therapies, immunotherapies, and even personalized approaches to impact the set of lesions. Additionally, the book discusses radiotherapy with regard to the many options available to treat patients using myriad fractionated techniques with various sources. Finally, Gliomas reviews issues specific to the quality of life for patients, and techniques for maximizing the effect of caregivers.
Edited and authored by premier researchers from around the world, Gliomas is a comprehensive reference for clinicians and researchers seeking the most up-to-date information on gliomas, and a guide to the best ways to effectively manage glioma patients and their care.
- Synthesizes widely dispersed information on the management of gliomas into one comprehensive resource
- Chapters written by international authors who are preeminent researchers in the field
- Fully explores the therapeutic options for patient care, from chemotherapy to radiotherapy to personalized approaches
Section 1
Diagnosis and treatment
Chapter 1
Epidemiology
Kyle M. Walsh1; Hiroko Ohgaki2; Margaret R. Wrensch1,* 1 Division of Neuroepidemiology, Department of Neurological Surgery, University of California San Francisco and UCSF Helen Diller Family Cancer Center, San Francisco, CA, USA
2 Section of Molecular Pathology, International Agency for Research on Cancer, Lyon, France
* Correspondence to: Margaret R. Wrensch, PhD, Department of Neurological Surgery, University of California, San Francisco, 1450 Third Street, Room HD273, San Francisco CA 94158, USA. Tel: + 1-415-476-1979 email address: [email protected]
2 Section of Molecular Pathology, International Agency for Research on Cancer, Lyon, France
* Correspondence to: Margaret R. Wrensch, PhD, Department of Neurological Surgery, University of California, San Francisco, 1450 Third Street, Room HD273, San Francisco CA 94158, USA. Tel: + 1-415-476-1979 email address: [email protected]
Abstract
More than 250 000 new cases of primary malignant brain tumors are diagnosed annually worldwide, 77% of which are gliomas. A small proportion of gliomas are caused by the inheritance of rare high-penetrance genetic variants or high-dose radiation. Since 2009, inherited genetic variants in 10 regions near eight different genes have been consistently associated with glioma risk via genome-wide association studies. Most of these variants increase glioma risk by 20–40%, but two have higher relative risks. One on chromosome 8 increases risk of IDH-mutated gliomas sixfold and another that affects TP53 function confers a 2.5-fold increased risk of glioma. Functions of some of the other risk variants are known or suspected, but future research will determine functions of other risk loci. Recent progress also has been made in defining subgroups of glioma based on acquired alterations within tumors. Allergy history has been consistently associated with reduced glioma risk, though the mechanisms have not yet been clarified. Future studies will need to be large enough so that environmental and constitutive genetic risk factors can be examined within molecularly defined, etiologically homogeneous subgroups.
Keywords
glioma; genetic epidemiology; risk factors; tumor genetics; environment; genome-wide association study; allergy; telomeres; survival; prognostic marker
Descriptive epidemiology1
Glioma incidence by age and histologic subtype
Primary malignant brain tumors are the 17th most common cancer type worldwide, with more than 250 000 new cases diagnosed annually (Forman et al., 2013). Approximately 77% of these are gliomas, which include pilocytic astrocytoma (World Health Organization (WHO) grade I), diffuse astrocytoma (WHO grade II), anaplastic astrocytoma (WHO grade III), glioblastoma (WHO grade IV), oligodendroglioma (WHO grade II), anaplastic oligodendroglioma (WHO grade III), ependymomas (WHO grade II), anaplastic ependymoma (WHO grade III), and mixed gliomas (Louis et al., 2007). In the USA more than 19 000 new cases of glioma are diagnosed each year with an age-adjusted average annual incidence rate of 6.24 per 100 000 population (Ostrom et al., 2014b). Brain tumor incidence rates have increased over the past three decades, with improved reporting, increased use of diagnostic imaging, and changing attitudes toward diagnosis in the elderly suspected to account for much of this observed increase (Ohgaki and Kleihues, 2005). Although primary brain tumors are relatively rare compared with metastatic brain tumors or more common primary cancer sites such as lung, breast, prostate, and colorectal, they constitute an important source of morbidity and mortality. In children, brain tumors cause one-quarter of all cancer deaths (Ostrom et al., 2015a).
The histologic distribution of glioma is very different in adults versus that observed in children (Fig. 1.1). Pilocytic astrocytoma (WHO grade I), the most common glioma in children, accounts for 37% of all glioma diagnoses among those under age 20 (Fig. 1.1A). Glioblastoma (WHO grade IV), the most common glioma in adults, accounts for 67% of all adult glioma diagnoses (Fig. 1.1B) (Ostrom et al., 2014b).
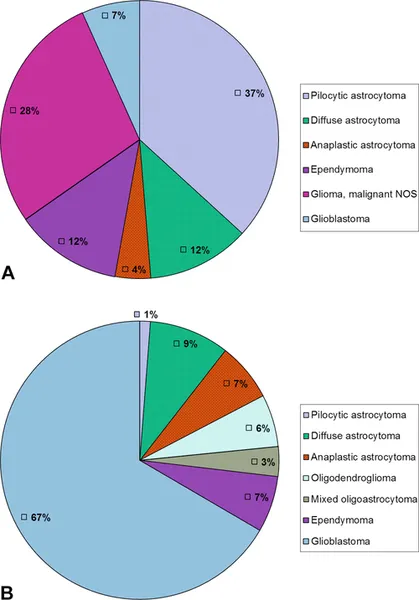
Fig. 1.1 Percentages of glioma by histologic type in children (A) and adults (B). NOS, not otherwise specified. (Data from Ostrom et al., 2014b, Table 19.)
The incidence rates of both pilocytic astrocytoma and ependymoma decrease throughout childhood and into adolescence (Fig. 1.2A). In adults, overall incidence of glioma dramatically increases with advancing age. However, the incidence of oligodendroglioma and ependymoma peaks in middle age and there is a decline in the incidence of glioblastoma among those 85 years and older (Fig. 1.2B) (Ostrom et al., 2014b). As with other cancers, the increased incidence of glioma with age could be due to the length of time required for malignant transformation, the necessity of many genetic alterations prior to the onset of clinical disease, and/or diminished immune surveillance.
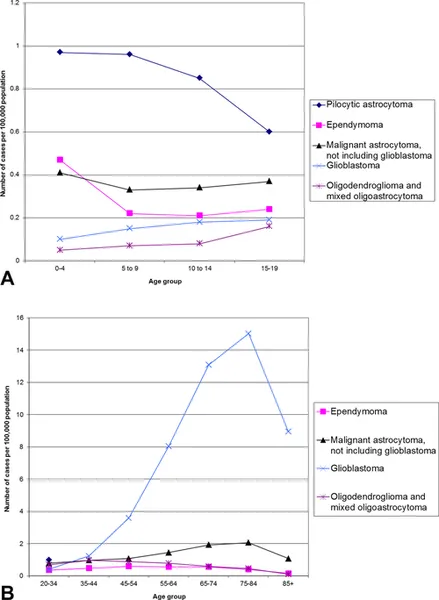
Fig. 1.2 Incidence of common glioma histologies by age at diagnosis, in children (A) and adults (B). (Data from Ostrom et al., 2014b, Tables 10 and 15, are age-adjusted to the 2000 US standard population.)
Differences in glioma incidence by sex, ethnicity, and geographic location
Men have higher incidences rates of glioma, embryonal tumors, germ cell tumors, and primary central nervous system (CNS) lymphoma, whereas women have higher incidence rates of meningioma and pituitary tumors. The 1.3-fold increased risk of glioma in males versus females is among the most consistent findings in brain tumor epidemiology (Ostrom et al., 2014b, 2015a). Because of the consistency of this finding, even in pediatric populations, a comprehensive understanding of glioma etiology must account for this observation. However, this important epidemiologic observation remains unexplained.
Interpretations of ethnic and geographic variation in the occurrence of brain tumors are complicated by problems in ascertainment and reporting. Regions with the highest reported rates of primary malignant brain tumors (e.g., Northern Europe, US white population, and Israel: rates of 11–20 per 100 000 population) generally have better access to medical imaging than areas with the lowest rates (e.g., India and the Philippines: rates of 2–4 per 100 000 people) (Inskip et al., 1995). However, some of the variation suggests ethnic differences in inherited susceptibility and/or cultural or geographic differences in risk factors (Jacobs et al., 2012; Dubrow et al., 2013). Most notably, the rate of malignant brain tumors in Japan, an economically prosperous country, is less than half the rate in Northern Europe (Forman et al., 2013). Furthermore, in the USA, whites have higher rates of glioma than African Americans but lower rates of meningioma (Fig. 1.3) (Ostrom et al., 2014b). These observations would be difficult to attribute solely to differences in access to medical care or diagnostic practices.
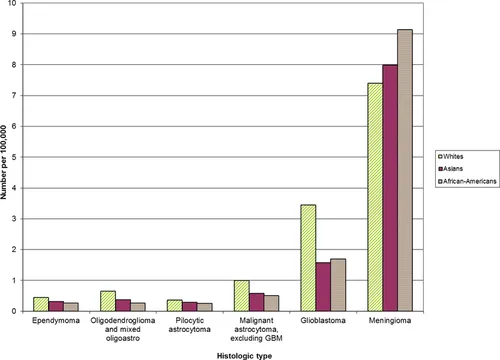
Fig. 1.3 Primary glioma and meningioma incidence, by ethnicity. (Data from Ostrom et al., 2014b, Table 4, are age-adjusted to the 2000 US standard population.)
The absolute variation in the occurrence of brain tumors between high-risk and low-risk areas is on the order of fourfold, compared with the 20-fold difference observed for lung cancer or the 150-fold difference observed for melanoma (Forman et al., 2013). Thus, for glioma, it seems unlikely that there are strong environmental risk factors associated with geography.
Incidence of molecular subgroups of glioma
Recent studies have focused on using molecular markers to help clarify glioma classification (Cancer Genome Atlas Research Network, 2008; Jiao et al., 2012; Liu et al., 2012; Brennan et al., 2013; Wiestler et al., 2013; Eckel-Passow et al., 2015; Mur et al., 2015; Spiegl-Kreinecker et al., 2015). For example, three acquired molecular alterations (IDH mutation, 1p19q co-deletion, and TERT promoter mutation) found in glioma tumor cells define five etiologically and clinically distinct groups of glioma patients that account for over 95% of grade II–IV gliomas (Eckel-Passow et al., 2015). Figure 1.4 shows the proportions of these molecular groups expected among incident infiltrating grade II–IV adult gliomas, estimated at the population level (Rice et al., 2015). Further work will help to establish the precise distribution and utility of these and other molecular classifications currently being considered.
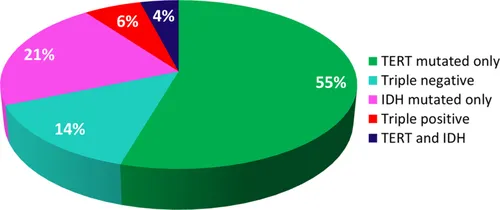
Fig. 1.4 Estimated distribution of five molecular groups of glioma based on presence or absence of TERT promoter mutation, IDH1/2 mutation, and 1p19q co-deletion among adults diagnosed with glioma annually in the USA.
Inherited risk factors for glioma
Inherited genetic pr...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Handbook of Clinical Neurology 3rd Series
- Foreword
- Preface
- Contributors
- Section 1: Diagnosis and treatment
- Section 2: Complications and symptomatic management
- Section 3: Disease-specific chapters
- Index
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Gliomas by in PDF and/or ePUB format, as well as other popular books in Medicine & Neurology. We have over 1.5 million books available in our catalogue for you to explore.