- 536 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Image-Guided Neurosurgery
About this book
Image-Guided Neurosurgery provides readers with an update on the revolutionary improvements in imaging and visualization relating to neurosurgery. From the development of the pneumoencephalogram, to the operating microscope, to cross sectional imaging with CT and later MRI, to stereotaxy and neuronavigation, the ability to visualize the pathology and surrounding neural structures has been the driving factor leading surgical innovation and improved outcomes.
The book provides a comprehensive reference on the application of contemporary imaging technologies used in neurosurgery. Specific techniques discussed include brain biopsies, brain tumor resection, deep brain stimulation, and more.
The book is ideal for neurosurgeons, interventional radiologists, neurologists, psychiatrists, and radiologists, as well as technical experts in imaging, image analysis, computer science, and biomedical engineering.
- A comprehensive reference on image-guided neurosurgery
- Includes coverage of neuronavigation in cranial surgery and advanced imaging, including functional imaging, adoption of intra-operative MRI and emerging technologies
- Covers all image-guided neurosurgery tools, including robotic surgical devices
- Ideal reference for topics relating to neurosurgery, imaging, stereotaxis, radiosurgery, radiology, epilepsy, MRI, the use of medical robotics, lasers, and more
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
Introduction and Historical Perspectives on Image-Guided Surgery
Robert L. Galloway, Jr., Center for Technology-Guided Surgery, Vanderbilt University, Nashville, TN, USA
This chapter traces the development of image-guided neurosurgery systems. The process is broken down into image acquisition, registration, localizers, and display. In addition the forces driving each step of the development are examined.
Keywords
image guidance; optical tracking; articulated arms; registration
While a number of dry reviews exist of the rise of image-guided neurosurgery (IGN), mine included,1–4 I find a discussion of why IGN came into being somewhat lacking. So, consider the brain as a surgical target. It is the only organ entirely encased in bone and it lacks redundancy. That is, the function of the tissue at one location is not replicated in other locations. Contrast this to a liver or a kidney. In addition, the value of any given section of brain is different from other similarly sized section of brain. Highly valued sections of brain tissue are referred to as “eloquent areas” and they can change from patient to patient depending on hand dominance, patient age, and existing disease. Thus, in considering the rise of IGN, one has to consider both the surgical target—tumor, vascular anomaly, or seizure foci—and the path to that target. A lack of guidance can lead to significant collateral damage of previously healthy functional tissue on the way to the surgical target. Rough guidelines embodied in the idea of standard approaches were an attempt to bring collective wisdom into the selection of surgical path. Implicit in these approaches is the thinking “bad things happen less often if you go this way” or “there is less damage to the average person’s anatomy if you use this approach.”
It was that generalization of anatomy which inspired Sir Victor Horsley and Robert Clarke to develop the first stereotactic frame,5 but also ultimately limited its value. Horsley and Clarke were interested in mapping brain function and (rightly) believed that function which lay in one area of the brain of a subject, such as dogs, cats and/or monkeys, would be reflected in similar locations in other subjects of the same species. They developed a gridding system in the form of a glass plate which they would lay over a sliced section of a freshly sacrificed animal of the same species and use those locations to provide coordinates in the living animal. An “electrolytic” needle was used to make small lesions. The estimated lesion location and the observed response of the subject were recorded. In addition, Clarke had developed a microtome for slicing excised brains and Horsley produced photographic albums of 1 to 2 mm thick cut sections in transverse, sagittal and coronal planes, presaging modern tomography by 70 years. In addition, they gave rise to the concept of a device existing external to the cranium being used to guide tools into the interior of the cranium.
The ultimate limitation of the work by Horsley and Clarke lies in the presumption that all subjects of similar size and same species will have corresponding internal and external anatomy. While Horsley and Clarke were able to produce lesions and occasionally get similar effects in their work, the variability of their results showed that the exterior of a subject did not correctly predict the interior of the subject. Their careers and standing in medical and scientific circles was such that, even given the variability of their animal results, the use of their frame in humans was proposed.6
With the exterior of the subject failing to predict the inside, stereotaxy had to wait for developments that allowed patient-specific information to be obtained. The first candidate was X-ray, but simple radiographs of the head resulted in skull images with no perceivable soft-tissue contrast. Dandy’s work on ventriculography7 (later called pneumoencephalography) allowed the delineation of the ventricles and therefore intuition of the location of space-occupying objects such as tumors or subdural hematomas. Moniz8 and others developed cerebral angiography in the 1930s and one of the other major structures, the cerebral vasculature and malformations thereof, could then be seen in radiographs.
Stereotactic Frames
By the 1940s radiography had progressed to the point that most of the subcerebral structures could be approximated if not seen. That, and injuries resulting from World War II, inspired Spiegel and Wycis9 to return to the concepts of stereotaxy. They developed a frame, affixed to the patient’s head with plaster and imaged using pneumoencephalography. However, for the most part, their targets were not cancer or vascular volumes but electrophysiological in nature:
This apparatus is being used for psychosurgery. In a series of patients studied in collaboration with H. Freed, lesions have been placed in the region of the medial nucleus of the thalamus (medial thalamotomy) in order to reduce the emotional reactivity by a procedure much less drastic than frontal lobotomy. The results so far obtained are promising. Further applications of the stereotaxic technic are under study, e.g. interruption of the spinothalamic tract in certain types of pain or phantom limb; production of pallidal lesions in involuntary movements; electrocoagulation of the Gasserian ganglion in trigeminal neuralgia; and withdrawal of fluid from pathological cavities, cystic tumors.
So their image-driven targeting did not have to be particularly fine. Their intent was to lesion problematic neural sites and they could use the placed electrode to refine their position.
Whether inspired by Spiegel and Wycis or driven by the same problems and opportunities, the late 1940s and early 1950s saw an explosion of stereotactic systems and techniques. These include systems by Leksell,10 Talairach,11 Reichert,12 and others. Most of these techniques were targeted toward electrophysiological procedures using electrophysiological measures for refinement of position. The rise (and subsequent fall) of stereotactic procedures was elegantly documented by Gildenberg13 (see Figure 1.1).
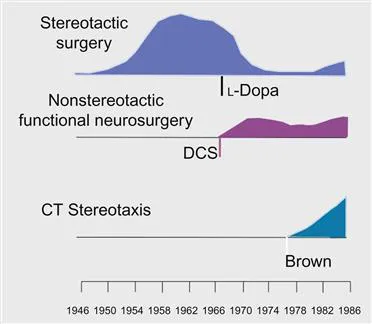
Since the majority of stereotactic cases were ultimately electrophysiological in nature, the development of antiseizure medications such as L-Dopa allowed diseases such as Parkinson’s disease to be treated without surgery—thus, the rapid decline in stereotactic cases. But the development and commercialization of a new form of imaging changed stereotaxy.
Advent of Volumetric Tomography
While it is difficult to define who exactly “invented” CT scanning, there is little question that the first commercially available system was invented in large part by Godfrey Hounsfield and developed by EMI (Electric and Music Industries) in 1972. With that development the imaging uncertainty of X-ray based imaging went from being the thickness of the patient’s head to millimeters in plane and a centimeter across planes. Contrast agents still had value but it was the improvement in the third dimension of visualization that was critical.
The availability of three-dimensional data was not lost on the stereotactic community but there was a lack of clarity as to how to make use of it. This was addressed when Russell Brown14 developed the simple but elegant N-localizer system. This system is shown in Figure 1.2.
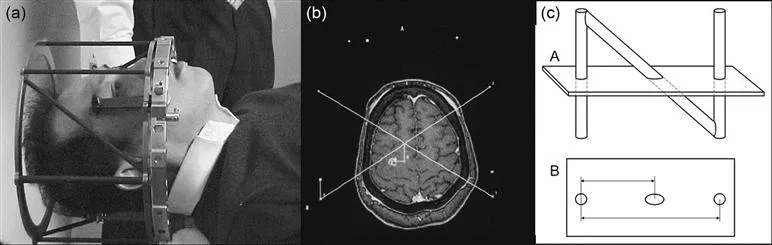
Because the X and Y location of any target could be visualized and the height above the base ring calculated, each image held the target coordinates. By having two lateral and one AP sets of N-bars, the orientation of the image plane could also be determined from any tomographic image in which the N-bars were visible.
It did not take the innovators in stereotactic surgery long to embrace the new technology. Leksell15 and Mundinger16 both published papers on using the new technology. Gildenberg17 even developed a technique for creating quasi-AP and Lateral images from CT so that surgeons with old calculation methods could use the images. But it was two surgeons with access to greater computational intensity who began to see the real value. By using the N-bars they could confirm the orientation and spacing of the CT slices. That allowed them to trust the volumetric nature of the scan and to use it not merely for neuroelectrical interventions but for volumetric resections. This work was led by Shelden18,19 and Kelly...
Table of contents
- Cover image
- Title page
- Table of Contents
- Copyright
- Dedication
- Foreword
- List of Contributors
- Chapter 1. Introduction and Historical Perspectives on Image-Guided Surgery
- Section I: Methods
- Section II: Applications
- Section III: New Directions
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Image-Guided Neurosurgery by Alexandra J. Golby in PDF and/or ePUB format, as well as other popular books in Medicine & Neurology. We have over 1.5 million books available in our catalogue for you to explore.