eBook - ePub
Bioactive Food as Dietary Interventions for Liver and Gastrointestinal Disease
Bioactive Foods in Chronic Disease States
- 802 pages
- English
- ePUB (mobile friendly)
- Available on iOS & Android
eBook - ePub
Bioactive Food as Dietary Interventions for Liver and Gastrointestinal Disease
Bioactive Foods in Chronic Disease States
About this book
Bioactive Food as Dietary Interventions for Liver and Gastrointestinal Disease provides valuable insights for those seeking nutritional treatment options for those suffering from liver and/or related gastrointestinal disease including Crohn's, allergies, and colitis among others. Information is presented on a variety of foods including herbs, fruits, soy and olive oil. This book serves as a valuable resource for researchers in nutrition, nephrology, and gastroenterology.
- Addresses the most positive results from dietary interventions using bioactive foods to impact diseases of the liver and gastrointestinal system, including reduction of inflammation, improved function, and nutritional efficiency
- Presents a wide range of liver and gastrointestinal diseases and provides important information for additional research
- Associated information can be used to understand other diseases, which share common etiological pathways
Trusted by 375,005 students
Access to over 1.5 million titles for a fair monthly price.
Study more efficiently using our study tools.
Information
Chapter 1
The Alkaline Way in Digestive Health
The biochemical consequences of diet are the greatest influence on overall metabolism for most patients. Food choices clearly affect the course of common pathophysiological errors such as insulin resistance, metabolic syndrome, and their sequella. However, these dynamics can also be considered a leverage point – an opportunity to reverse immune reactivity through practical interventions that patients can implement in their daily lives.
1 Dietary Factors in Metabolism
The intestinal tract plays a key part in nutrient absorption, immune defense against foreign invaders, physiologic repair from wear and tear, growth, neurohormone regulation and stress management. Disorders anywhere in the gastrointestinal system can affect the function of the entire body and overall health. Digestive competence tends to predict survival and the capacity to thrive years to decades later.
1.1 Profile: Metabolic Acidosis as a Major Cause of Chronic Disease
Toxin accumulation in the body can result from a diet that promotes metabolic acidosis (net acid excess after metabolism) as shown by low levels of buffering minerals such as potassium and magnesium. A number of large research studies involving thousands of participants have reported about the association between metabolic acidosis and insulin resistance (Jaffe and Mani, 2006; Souto et al., 2011), type 2 diabetes (Jaffe and Mani, 2006; Schulze et al., 2003), cardiometabolic risk (Murakami et al., 2008), coronary heart disease (Liu et al., 2000), and osteoporosis (Jaffe and Brown, 2000; Jehle et al., 2006), as well as cancer (Tavani et al., 2000). A typical American diet provides insufficient minerals and fiber to counter or buffer the buildup of metabolic acids and to help displacement of toxic wastes. As a result, alkaline cellular reserves within the body reduce and deplete as the intracellular environment becomes progressively acidic, mineral depleted and proton rich (Lim, 2007; Zeidel and Seifter, 1986).
1.1.1 Associated signs and symptoms
The symptoms associated with metabolic acidosis include malaise and fatigue, metabolic syndrome and diabetes, osteopenia and osteoporosis, and depression. Metabolic acidosis is associated with a broad range of clinical conditions in the body because of the biochemical reduction of the proton gradient, upon which cell energy depends. The ratio of ATP: ADP is a measure of cell energy. A ratio of 100:1 is healthy. A ratio less than 80 begins to shift cells from an elective protective, proactive, and prevention mode to a survival mode.
1.1.1.1 Fatigue
Low energy is the major complaint that patients report to their primary care physician. Energy production and the ability to remove toxins safely are compromised when even minor increases in acidity occur. Metabolic acidosis has also been linked to chronic fatigue immune dysfunction syndrome (Jaffe and Brown, 2000). Fibromyalgia and chronic muscle pain that is unresponsive to pain medication have been documented to produce acidic end products that directly irritate and inflame nerve muscle end plates (Deuster and Jaffe, 1998). We observe restoration of vitality and quality of life when metabolic acidosis is corrected comprehensively using predictive tests compared to best outcome reference ranges thus incorporating personalized biochemical individuality into primary care.
1.1.1.2 Osteopenia and osteoporosis
Excess acid within the cells is also a key factor in osteoporosis (Maurer et al., 2003). One of the best examples of this metabolic sensitivity is the influence of acid–alkali balance on skeletal structure, health, and integrity. Skeletal muscles are the largest storehouse of available minerals in the body and are thus exquisitely sensitive to small changes in pH. Even a 10% reduction in pH increases osteoclastic activity while inhibiting osteoblastic function, inducing amplified bone mineral loss (Jehle et al., 2006). For the past 20 years, we have consistently observed 2–10% new bone growth confirmed by DEXA scores after just 2 years.
1.1.2 Relevant evaluations
One of the most useful assessments in the management of metabolic acidosis is self-testing for pH, which can be performed simply by the patient in their home. After 6 h of rest, we find the urine pH is equilibrated with the urinary tract cells. Costing pennies per day, this is a useful self-care test that motivates better compliance with healthier choices. Another assessment involves laboratory testing for reactive food antigens. In tandem, these tests can be pivotal in correcting metabolic acidosis and repair deficits often called inflammation and their myriad sequellae.
1.1.2.1 Self-evaluation: Testing for pH
The hazard of metabolic acidosis is that it requires additional minerals to buffer and remove excess acids from the body, stripping out needed minerals with potential harm to the kidneys and urinary tract. The role of metabolic acidosis in chronic kidney disease has been extensively documented (Sahni et al., 2010).
A pH assessment of the first morning urine provides a clinically useful measure of metabolic acidosis risk. The urine pH is a predictive indicator of the body’s mineral reserves, as well as acid/alkaline status (Whiting and Bell, 2002). Typically pH balance is restored during sleep and rest when excess acids are excreted (Shafiee et al., 2002). This capacity varies widely based on the specific toxic load and the individual’s ability to make energy, deactivate toxins, and excrete those toxins as reported by Bazhin (2007) (see Figure 1.1, pH strips and Figure 1.2, reference range for urine measurement).

Figure 1.1 Picture of pH strips.
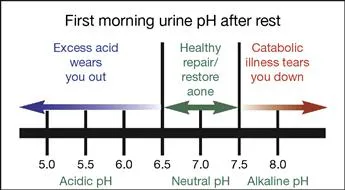
Figure 1.2 Interpretation of first, morning-urine measurements.
A value of 7.0 indicates a neutral state, a balance of acid, and alkaline elements. The first morning urine pH goal of 6.5–7.5 shows healthy mineral balance. Neutral or low-level acid excess reflected in lower pH values indicates that metabolic chemistry is appropriately alkaline and that the small amounts of metabolic acids built up from daily metabolism have been easily concentrated and excreted. Cell cytoplasm or ‘cell juice’ functions in an exquisitely narrow, slightly alkaline optimum functional pH range (De Young, 1994; Zeidel and Seifter, 1986).
1.1.2.2 Laboratory evaluation: Reducing immune reactivity
Immune responses directly and indirectly generate substantial amounts of acidic products. For the at-risk individual with impaired dietary buffering capacity, it is especially important to avoid immune reactions due to antigen reactivity or other causes that can contribute to additional cell acidity in the system (Jaffe et al., 2006). A lymphocyte response assay (LRA) can identify delayed allergic reactivity. Substitution of immune reactive substances lowers acid loads.
1.1.3 Clinical interventions: the alkaline way
Reduction of hyperacidity in the body can be achieved through a nutrient-rich alkaline diet, targeted supplementation with alkaline nutrients, and the inclusion of buffered fats.
1.1.3.1 Alkaline diet
The Alkaline Way diet is a health-promoting, fiber-rich diet that consists primarily of whole foods based on individual food tolerances and sensitivities. Preference is given to locally, vine-ripened, organic, or biodynamic sources of foods. Mineral-rich water is the preferred beverage. Reducing the net excess cell acidity supports a range of health benefits.
1.1.3.1.1 Enhancing immune defenses
Alkalinizing foods improve immune defense and repair functions (Lee and Shen, 2008) by reducing host hospitality to chronic infections. This reduced infectious challenge results in lower levels of inflammation, more resources for anticancer surveillance, and enhanced repair capacity. Clinical strategies that accompany an alkaline diet include a rotation or a substitution diet to reduce exposure to reactive foods coupled with health-promoting food choices, fresh fruits and vegetables, pulses and grasses, whole grains, minimal animal protein, and a program of individualized nutritional supplements to fully meet biochemical needs.
1.1.3.1.2 Buffering cellular chemistry
A metabolically alkaline diet means that food has a buffering or cell acid neutralizing effect on in vivo cellular chemistry, in vivo (Budde and Crenshaw, 2003). The effects of specific food responses within the body can differ from that food’s test tube chemistry (Gonick et al., 1968). For example, citrus fruits are alkalinizing in the body because citrate, malate, succinate, and fumarate all promote the generation of more than twice as much bicarbonate as the acid contributed from the total amount of food metabolized (Brown and Trivieri, 2006). This means that citrus fruits and similar foods are acidic in a test tube environment, yet alkaline forming in the body.
Figure 1.3 reflects this real-time perspective on metabolism – assessing nutrition for in vivo efficacy rather than merely evaluating the ash residue of the food as has been historically performed in nutrient assays. The foods listed here are categorized based on an empirical formula calculated from the actual composition of the foods’ total protein, fat, carbohydrates, minerals, cofactors, and fiber contents (Jaffe, 1987).
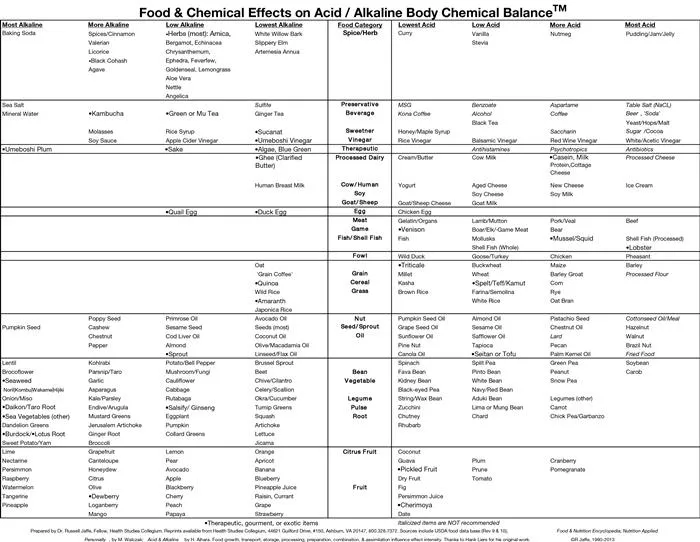
Figure 1.3 Food and chemical effects on acidic/alkaline body chemical balance.
1.1.3.2 Alkaline nutrients
A diet high in acidic foods tends to be less-nutrient-dense and fiber-rich than an alkaline forming, whole foods, immune tolerant diet. Once mineral depletion occurs, cells become progressively more acidic and less energetic. The cell cytoplasm proton gradient is required for the cellular power centers, mitochondria, to work effectively. When the cell becomes acidic, the proton gradient is reduced and cells become dependent on anaerobic “survival” metabolism. This is a less...
Table of contents
- Cover image
- Title page
- Table of Contents
- Acknowledgments for Bioactive Foods in Chronic Disease States
- Copyright
- Preface: Liver and Gastrointestinal Health
- Contributors
- Chapter 1. The Alkaline Way in Digestive Health
- Chapter 2. Functional Assessment of Gastrointestinal Health
- Chapter 3. Antioxidants in Inflammatory Bowel Disease, Ulcerative Colitis, and Crohn Disease
- Chapter 4. Omega-6 and Omega-3 Polyunsaturated Fatty Acids and Inflammatory Bowel Diseases
- Chapter 5. Alcohol and Gastrointestinal Tract Function
- Chapter 6. Dangerous Herbal Weight-Loss Supplements
- Chapter 7. Milk Bacteria: Role in Treating Gastrointestinal Allergies
- Chapter 8. Nutritional Functions of Polysaccharides from Soy Sauce in the Gastrointestinal Tract
- Chapter 9. Nutrition, Dietary Fibers, and Cholelithiasis: Cholelithiasis and Lipid Lowering
- Chapter 10. Indian Medicinal Plants and Spices in the Prevention and Treatment of Ulcerative Colitis
- Chapter 11. Ginger (Zingiber officinale Roscoe): An Ancient Remedy and Modern Drug in Gastrointestinal Disorders
- Chapter 12. The Role of Microbiota and Probiotics on the Gastrointestinal Health: Prevention of Pathogen Infections
- Chapter 13. Probiotics and Irritable Bowel Syndrome
- Chapter 14. Antioxidant, Luteolin Exhibits Anti-inflammatory Effect in In Vitro Gut Inflammation Model
- Chapter 15. Human Microbiome and Diseases: A Metagenomic Approach
- Chapter 16. Folate Production by Lactic Acid Bacteria
- Chapter 17. Probiotics against Digestive Tract Viral Infections
- Chapter 18. Probiotic Bacteria as Mucosal Immune System Adjuvants
- Chapter 19. Medicinal Plants as Remedies for Gastrointestinal Ailments and Diseases: A Review
- Chapter 20. Review on the Protective Effects of the Indigenous Indian Medicinal Plant, Bael (Aegle marmelos Correa), in Gastrointestinal Disorders
- Chapter 21. Gastrointestinal and Hepatoprotective Effects of Ocimum sanctum L. Syn (Holy Basil or Tulsi): Validation of the Ethnomedicinal Observation
- Chapter 22. Turmeric (Curcuma longa L.) the Golden Curry Spice as a Nontoxic Gastroprotective Agent: A Review
- Chapter 23. Nutrition, Dietary Fibers, and Cholelithiasis: Apple Pulp, Fibers, Clinical Trials
- Chapter 24. Gastrointestinal Protective Effects of Eugenia jambolana Lam. (Black Plum) and Its Phytochemicals
- Chapter 25. Preventing the Epidemic of Non-Communicable Diseases: An Overview
- Chapter 26. Omega 3 Fatty Acids and Bioactive Foods: From Biotechnology to Health Promotion
- Chapter 27. Carotenoids: Liver Diseases Prevention
- Chapter 28. Omega-3 Fatty Acids and Early Life Nutritional Programming: Lessons from the Avian Model
- Chapter 29. Prebiotics, Probiotics, and Health Promotion:: An Overview
- Chapter 30. Gastroprotective Effects of Bioactive Foods
- Chapter 31. Antioxidant Activity of Anthocyanins in Common Legume Grains
- Chapter 32. Antioxidant Capacity of Pomegranate Juice and Its Role in Biological Activities
- Chapter 33. Dietary Bioactive Functional Polyphenols in Chronic Lung Diseases
- Chapter 34. Antioxidant Capacity of Medicinal Plants
- Chapter 35. Chinese Herbal Products in the Prevention and Treatment of Liver Disease
- Chapter 36. Bioactive Foods and Supplements for Protection against Liver Diseases
- Chapter 37. The Role of Prebiotics in Gastrointestinal and Liver Diseases
- Chapter 38. The Role of Curcumin in Gastrointestinal and Liver Diseases
- Chapter 39. Toll-Like Receptors and Intestinal Immune Tolerance
- Chapter 40. Psychological Mechanisms of Dietary Change in Adulthood
- Chapter 41. Biochemical Mechanisms of Fatty Liver and Bioactive Foods: Fatty Liver, Diagnosis, Nutrition Therapy
- Chapter 42. Hepatoprotective Effects of Zingiber officinale Roscoe (Ginger): A Review
- Chapter 43. Betel Leaf (.0Piper betel Linn): The Wrongly Maligned Medicinal and Recreational Plant Possesses Potent Gastrointestinal and Hepatoprotective Effects
- Chapter 44. Hepatoprotective Effects of Picroliv: The Ethanolic Extract Fraction of the Endangered Indian Medicinal Plant Picrorhiza kurroa Royle ex. Benth
- Chapter 45. Scientific Validation of the Hepatoprotective Effects of the Indian Gooseberry (Emblica officinalis Gaertn): A Review
- Chapter 46. Biochemical Mechanisms of Fatty Liver and Bioactive Foods: Wild Foods, Bioactive Foods, Clinical Trials in Hepatoprotection
- Chapter 47. Phytochemicals Are Effective in the Prevention of Ethanol-Induced Hepatotoxicity: Preclinical Observations
- Index
Frequently asked questions
Yes, you can cancel anytime from the Subscription tab in your account settings on the Perlego website. Your subscription will stay active until the end of your current billing period. Learn how to cancel your subscription
No, books cannot be downloaded as external files, such as PDFs, for use outside of Perlego. However, you can download books within the Perlego app for offline reading on mobile or tablet. Learn how to download books offline
Perlego offers two plans: Essential and Complete
- Essential is ideal for learners and professionals who enjoy exploring a wide range of subjects. Access the Essential Library with 800,000+ trusted titles and best-sellers across business, personal growth, and the humanities. Includes unlimited reading time and Standard Read Aloud voice.
- Complete: Perfect for advanced learners and researchers needing full, unrestricted access. Unlock 1.5M+ books across hundreds of subjects, including academic and specialized titles. The Complete Plan also includes advanced features like Premium Read Aloud and Research Assistant.
We are an online textbook subscription service, where you can get access to an entire online library for less than the price of a single book per month. With over 1.5 million books across 990+ topics, we’ve got you covered! Learn about our mission
Look out for the read-aloud symbol on your next book to see if you can listen to it. The read-aloud tool reads text aloud for you, highlighting the text as it is being read. You can pause it, speed it up and slow it down. Learn more about Read Aloud
Yes! You can use the Perlego app on both iOS and Android devices to read anytime, anywhere — even offline. Perfect for commutes or when you’re on the go.
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Please note we cannot support devices running on iOS 13 and Android 7 or earlier. Learn more about using the app
Yes, you can access Bioactive Food as Dietary Interventions for Liver and Gastrointestinal Disease by Ronald Ross Watson,Victor R Preedy,Victor R. Preedy in PDF and/or ePUB format, as well as other popular books in Technology & Engineering & Human Anatomy & Physiology. We have over 1.5 million books available in our catalogue for you to explore.